
Ventricular Tachycardia Ablation at HRHF Clinic
From idiopathic VT in a structurally normal heart to scar-mediated VT, ARVC, HCM, and epicardial circuits — every type of ventricular tachycardia, treated with the right tools, by an experienced electrophysiologist.
Complete VT programme — western India
High procedural volume Carto 3D PASO Confidense · Bipolar & epicardial ablation routinely performed
-
Re-do VT cases & complex substrates welcome.
What is VT — and Why Does it Need Specialist Care?
Ventricular tachycardia — VT — is a fast heart rhythm that originates from the lower chambers of the heart. Unlike SVT, which arises from the upper chambers and is rarely life-threatening, VT is a more serious arrhythmia that always deserves expert evaluation.
But the word VT covers a very wide range of conditions. At one end of the spectrum is idiopathic VT — VT that occurs in a structurally normal heart, often in young people, and is generally not dangerous. At the other end is scar-mediated VT in patients with previous heart attacks or cardiomyopathy, where the arrhythmia can be life-threatening and requires urgent expert treatment.
The first step in any VT evaluation is determining which type you have. The treatment, the urgency, and the prognosis are all very different depending on the substrate. At HRHF Clinic, this evaluation is done thoroughly, calmly, and with the full diagnostic toolkit — so that the right treatment is offered for the specific type of VT you have.

The reassurance most VT patients need to hear
Many patients arrive frightened, often after an ICD shock, believing they have a uniformly grave condition. The reality is more nuanced. With accurate substrate diagnosis and modern ablation, even the most challenging VT can usually be controlled — and in many cases, eliminated. The first conversation should not be about prognosis. It should be about understanding what you have and what can be done.
The Right Technology for the Right VT
VT ablation requires more than a single tool. Different VT substrates need different mapping techniques, different ablation strategies, and sometimes different access routes. HRHF Clinic offers the complete toolkit — used routinely, not occasionally.
| Technology | What it does |
|---|---|
| Carto 3D Mapping | 3D electroanatomic mapping — reconstructs heart's electrical anatomy, identifies scar zones, precise targeting. |
| PASO Software | Pace-mapping integrated within Carto — compares paced beat morphology to clinical VT, identifies exit site. |
| Confidense Mapping | High-density multipolar mapping — thousands of points, detailed substrate information for scar VT & ARVC. |
| Bipolar Ablation | Two electrodes (endocardial + epicardial/contralateral) — essential for deep intramural circuits (HCM, septal scar). |
| Epicardial Mapping & Ablation | Sub‑xiphoid access to epicardial space — routine for ARVC, HCM, idiopathic epicardial VT, re‑do scar VT. |
| High‑Density Catheters | PentaRay, HD Grid — faster mapping, better resolution, complete substrate characterisation. |
-
Case in Focus — Bipolar Ablation
An Idiopathic VT That Could Not Be Reached From One Side
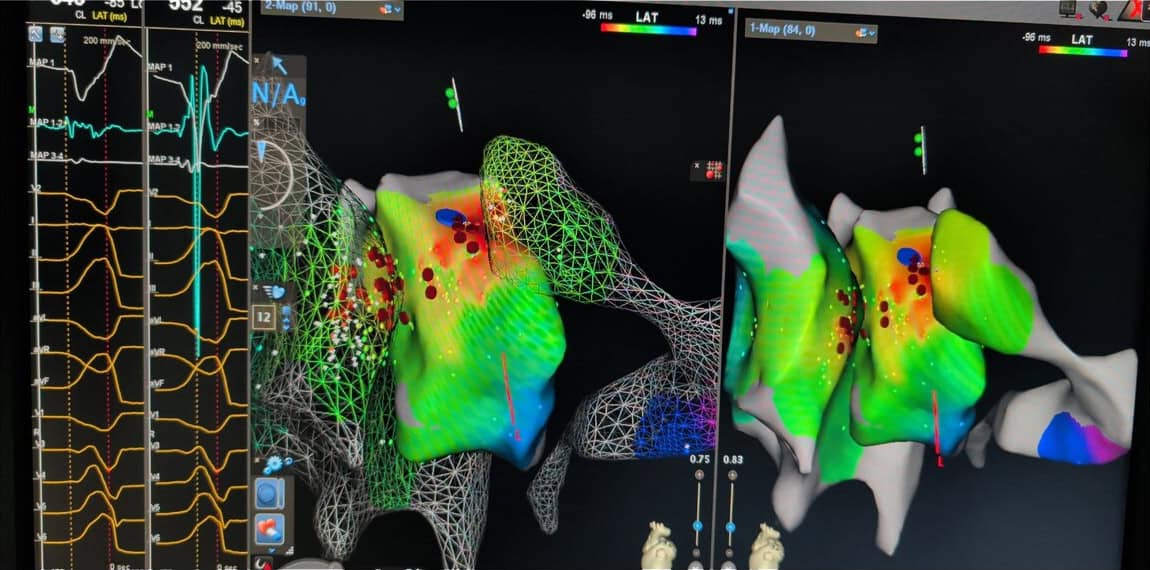
This patient had a symptomatic outflow tract VT with deep intramural origin between the right and left ventricular outflow tracts — a substrate where conventional ablation from either chamber alone often fails. Carto activation mapping identified earliest activation at the RVOT-LVOT interface; bipolar ablation was performed with one catheter in the RVOT and one in the LVOT, delivering energy across the intervening myocardium.
Five Substrates. Five Approaches. One Programme.
Each type of VT has a distinct cause, distinct mapping requirements, and distinct ablation strategy. The sections below cover the five major substrates we treat at HRHF Clinic — what each one is, what to expect, and how we approach treatment.
Idiopathic VT
Generally not dangerous · Excellent ablation outcomes
For Patients
Idiopathic VT is ventricular tachycardia that occurs in a heart that is otherwise structurally normal — no scar, no weakened muscle, no genetic disease. The heart pumps well, the valves are normal, the arteries are clear. The VT arises from a single focal site, most commonly the right or left ventricular outflow tract or the fascicles of the left bundle. This is generally a benign condition that does not shorten life expectancy. But it can cause significant symptoms — palpitations, breathlessness, dizziness — and can be very effectively cured with ablation.
If you have been diagnosed with idiopathic VT, the most important message is reassurance. Your heart is normal. The arrhythmia is treatable. Ablation in expert hands cures idiopathic VT in over 90 percent of cases — and even technically demanding cases that originate deep within the muscle between the two outflow tracts can now be successfully ablated using bipolar techniques.
Our Approach — Technology and Technique
Idiopathic VT mapping uses PASO pace-matching extensively — because the VT may not be sustained long enough for activation mapping, we reproduce the VT morphology by pacing from each candidate site and identify the location whose paced beat most closely matches the clinical VT. Carto provides the 3D anatomical context.
For most idiopathic VTs, focal radiofrequency ablation at the earliest activation point eliminates the arrhythmia. For deep intramural circuits between the right and left outflow tracts — historically very difficult to ablate — we use bipolar ablation with one catheter in the RVOT and one in the LVOT, delivering energy across the intervening myocardium.
Scar-Mediated VT
Serious · Requires expert evaluation · Highly treatable with modern ablation
For Patients
Scar-mediated VT is ventricular tachycardia that arises from areas of damaged or fibrotic heart muscle — most commonly after a previous heart attack, but also in patients with cardiomyopathy of any cause. The scar tissue itself does not conduct, but channels of surviving muscle running through the scar can act as the slow-conduction zone of a reentry circuit, sustaining the VT.
This is the substrate most patients fear — and it does require serious expert care. But modern ablation has transformed outcomes for scar VT. With proper substrate mapping, the channels within the scar can be identified and eliminated. Many patients who have suffered repeated ICD shocks become shock-free after a successful scar VT ablation.
If you have an ICD and have had VT episodes — even if you are currently on medications — a discussion about ablation may be appropriate. Modern guidelines support ablation as first-line therapy for many scar VT patients, ahead of escalating anti-arrhythmic drugs.
Our Approach — Technology and Technique
Scar VT mapping requires high-density substrate definition. We use Confidense mapping with multipolar catheters to acquire thousands of points across the affected chamber, identifying the precise location and architecture of scar zones, channels, and late potentials.
The ablation strategy depends on the individual circuit — sometimes targeting the critical isthmus during sustained VT (entrainment-guided), sometimes ablating all identified channels and late potentials (substrate-based), often a combination. PASO software supports identification of the VT exit site when activation mapping cannot be performed.
For deep intramural circuits unreachable from one surface, bipolar ablation between endocardial and epicardial catheters provides the depth needed.
ARVC VT
Genetic substrate · Often requires epicardial access · Specialist programme essential
For Patients
Arrhythmogenic Right Ventricular Cardiomyopathy — ARVC — is a genetic disease in which the right ventricle progressively develops fibrofatty scar, particularly in the epicardial layers. VT in ARVC arises from these fibrofatty regions and is often a presenting feature of the disease. ARVC can affect young people, including athletes, and the diagnosis often comes as a shock.
If you have been diagnosed with ARVC, you are likely under the care of a cardiologist who has discussed an ICD and exercise restrictions. What may not have been discussed is that VT ablation in ARVC has improved dramatically in the last decade — particularly when epicardial access is part of the strategy. Many ARVC patients can have their VT burden significantly reduced or eliminated, allowing them to live with fewer ICD shocks and a better quality of life.
Our Approach — Technology and Technique
ARVC VT typically requires both endocardial and epicardial mapping — because the substrate is predominantly epicardial in this condition, endocardial-only ablation often fails. We routinely perform sub-xiphoid epicardial access for ARVC ablation.
Carto Confidense mapping defines the substrate on both surfaces; the epicardial map characteristically shows extensive low-voltage areas with scattered late potentials in the right ventricular free wall. Ablation targets all abnormal substrate — late potentials, fractionated electrograms, channels — across endocardial and epicardial surfaces. This is technically demanding work and not routinely available outside high-volume EP centres.
Epicardial VT
Requires sub-xiphoid access · Performed routinely at HRHF Clinic
For Patients
Some VT circuits originate from the outer surface of the heart — the epicardium — rather than the inner chamber. These epicardial circuits cannot be reached from inside the heart, and conventional endocardial ablation will fail to eliminate them. This is a recognised reason for ablation failure at centres that do not perform epicardial access.
Epicardial ablation involves a small puncture below the breastbone, through which a thin catheter is advanced into the pericardial space — the thin sac surrounding the heart. From here, the outer surface of the heart can be mapped and ablated. The procedure is performed under sedation, takes approximately 2 to 3 hours in addition to standard endocardial mapping, and has a well-established safety profile in experienced hands.
Epicardial access is part of routine practice at HRHF Clinic — used for ARVC, HCM, idiopathic VT with epicardial origin, and re-do scar VT where endocardial ablation has previously failed. If you have been told that your VT cannot be ablated, or that a previous ablation has failed, an epicardial approach may be the answer.
Our Approach — Technology and Technique
Sub-xiphoid percutaneous epicardial access uses the technique pioneered by Sosa and colleagues — a needle puncture into the pericardial space under fluoroscopic guidance, followed by sheath placement and catheter advancement. We perform this routinely at HRHF Clinic, with the same Carto mapping system used endocardially.
Mapping and ablation strategies are the same as endocardial — voltage mapping, late potential identification, activation or PASO mapping during VT, and lesion delivery — but on the epicardial surface. Pre-procedure coronary angiography is performed when ablation will be near major coronary vessels.
The combination of routine endocardial-epicardial mapping is what allows HRHF Clinic to treat VT substrates that other centres decline.
HCM VT
Complex substrate · May require bipolar or epicardial ablation · Increasingly treatable
For Patients
Hypertrophic Cardiomyopathy — HCM — is a genetic disease causing thickening of the heart muscle. VT in HCM has historically been considered very difficult to ablate, and many HCM patients with recurrent VT have been managed primarily with ICDs and anti-arrhythmic drugs. This is changing.
With advances in mapping technology, bipolar ablation, and epicardial access, VT in HCM can now be successfully ablated in selected patients — particularly those with apical aneurysms, mid-cavity obstruction with apical scar, or focal scar substrate. HRHF Clinic has experience treating HCM VT, including patients with apical aneurysms — a recognised high-risk subgroup.
If you have HCM and have had VT episodes or appropriate ICD shocks, a discussion about ablation may be worthwhile — even if you have been told previously that ablation is not an option.
Our Approach — Technology and Technique
HCM VT often involves deep intramural circuits within thickened, scarred myocardium — substrates that conventional unipolar endocardial ablation cannot reach. Our approach combines:
- Detailed substrate mapping with Carto Confidense to identify scar and channels
- PASO pace-matching where activation mapping is not feasible
- Bipolar ablation for deep septal or intramural circuits
- Epicardial access for circuits that cannot be eliminated from the endocardium alone — particularly relevant in HCM with apical aneurysm
The VT Ablation Journey — Pre-procedure to Recovery
-
Pre‑procedure
Detailed review of your VT history, ECGs, ICD interrogation if applicable, imaging including echocardiogram and cardiac MRI when indicated. Discussion of substrate, ablation strategy, expected outcomes, and risks. Anti-arrhythmic drug adjustments if needed
-
Day of procedure
Admission in the morning. Final review and consent. Procedure performed under sedation in the EP lab. Standard procedure time: 3 to 6 hours depending on substrate and complexity. Endocardial mapping; epicardial access if indicated; substrate definition; ablation; testing for non-inducibility.
-
Recovery
Bed rest for several hours after the procedure. Most patients eat and walk by the evening. Telemetry overnight.
-
Discharge
Typically the day after the procedure for endocardial-only ablation; one additional night for procedures involving epicardial access. Discharge with instructions on activity, medication, and follow-up.
-
First Follow‑up
Two weeks after discharge — wound check, ICD interrogation, symptom review. Subsequent follow-up at 3 months, 6 months, 12 months — and as needed.
-
Long-term
Ongoing follow-up with your referring cardiologist for the underlying condition. We remain available for any VT-related concerns. ICD therapy, anti-arrhythmic drugs, and other treatments are reviewed at each visit and adjusted based on your response
Referring Your VT Patient
VT ablation is the most technically demanding subspecialty in clinical electrophysiology. Outcomes correlate strongly with operator volume, mapping technology, and the willingness to perform epicardial access when needed. HRHF Clinic offers all three.We accept VT referrals from across western India, with same working day acknowledgement and direct contact with Dr. Dhopeshwarkar for clinical discussion before referral. Re-do cases — patients with failed prior VT ablation elsewhere — are particularly welcome, as these are often the cases where epicardial mapping and bipolar ablation make the difference.
Refer for Ablation Evaluation
-
Recurrent ICD shocks despite optimal medical therapy
-
VT storm — three or more sustained VT episodes within 24 hours
-
Symptomatic idiopathic VT with structurally normal heart
-
Scar VT with appropriate ICD therapies — ablation as first-line consideration
-
ARVC with documented VT episodes — endo-epicardial mapping recommended
-
HCM with VT — including patients with apical aneurysm or mid-cavity obstruction
-
Failed prior VT ablation — re-do with epicardial access if not previously performed
-
VT with intolerance to amiodarone or other anti-arrhythmic drugs
-
Tachycardia-mediated cardiomyopathy from sustained or incessant VT
Common Questions About VT and VT Ablation
No. The danger of VT depends entirely on the substrate. Idiopathic VT in a structurally normal heart is generally not life-threatening. Scar VT in a patient with prior heart attack or cardiomyopathy is potentially serious. The first step is establishing which type you have.
Possibly yes. Recurrent ICD shocks have a real impact on quality of life and on long-term outcomes. Modern guidelines support ablation as first-line therapy for many patients with appropriate ICD therapies. A pre-procedure consultation can determine whether ablation is appropriate for you.
AF ablation has a favourable safety profile in experienced hands. Main risks include vascular access complications, cardiac tamponade (rare), oesophageal injury (rare with vHPSD), and stroke (rare). All risks are discussed in detail pre-procedure.
Most patients are back to normal activities within a week. Driving restrictions may apply if you have an ICD or have had documented VT — your team will discuss this. Avoid heavy lifting for two weeks. Wound care is straightforward.
Yes — almost always. Ablation reduces the burden of VT episodes but does not change the underlying substrate or the risk of future events. The ICD remains for protection. Many patients who had frequent shocks pre-ablation become shock-free post-ablation, but the ICD is retained.
If you have been told your VT cannot be ablated — speak to us first
HRHF Clinic offers the complete VT ablation programme in western India — including epicardial access, bipolar ablation, and re-do procedures. Direct access to Dr. Dhopeshwarkar for pre-referral discussion.