Two Patients. Two Locations. The Same Cure.
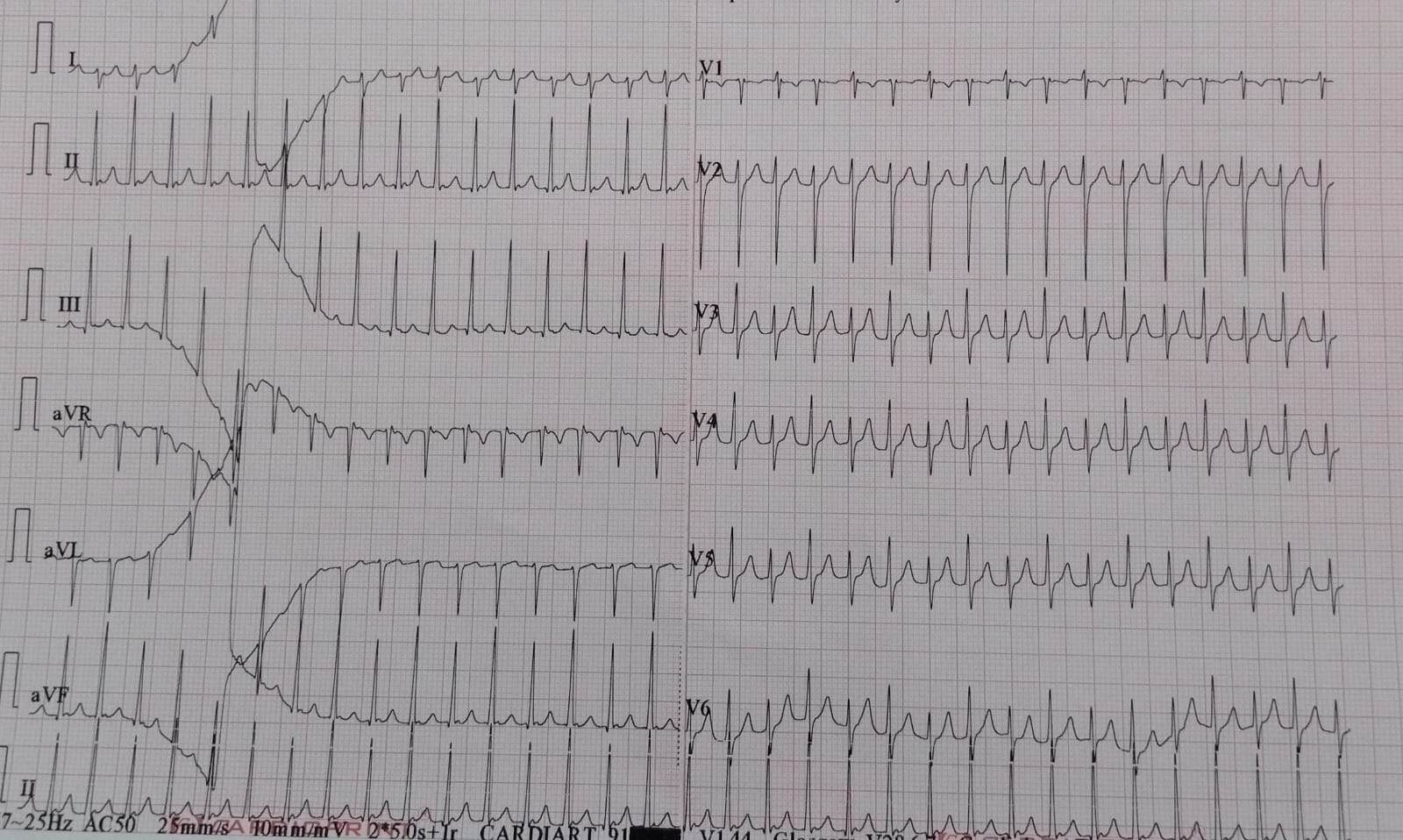
Not all SVTs come from the same place. Some arise from extra electrical connections (accessory pathways) along the mitral valve on the left side of the heart; others from the tricuspid valve on the right. Some pathways are visible on a routine ECG; others — concealed pathways — only conduct backwards and are invisible until specific mapping is performed during the procedure.
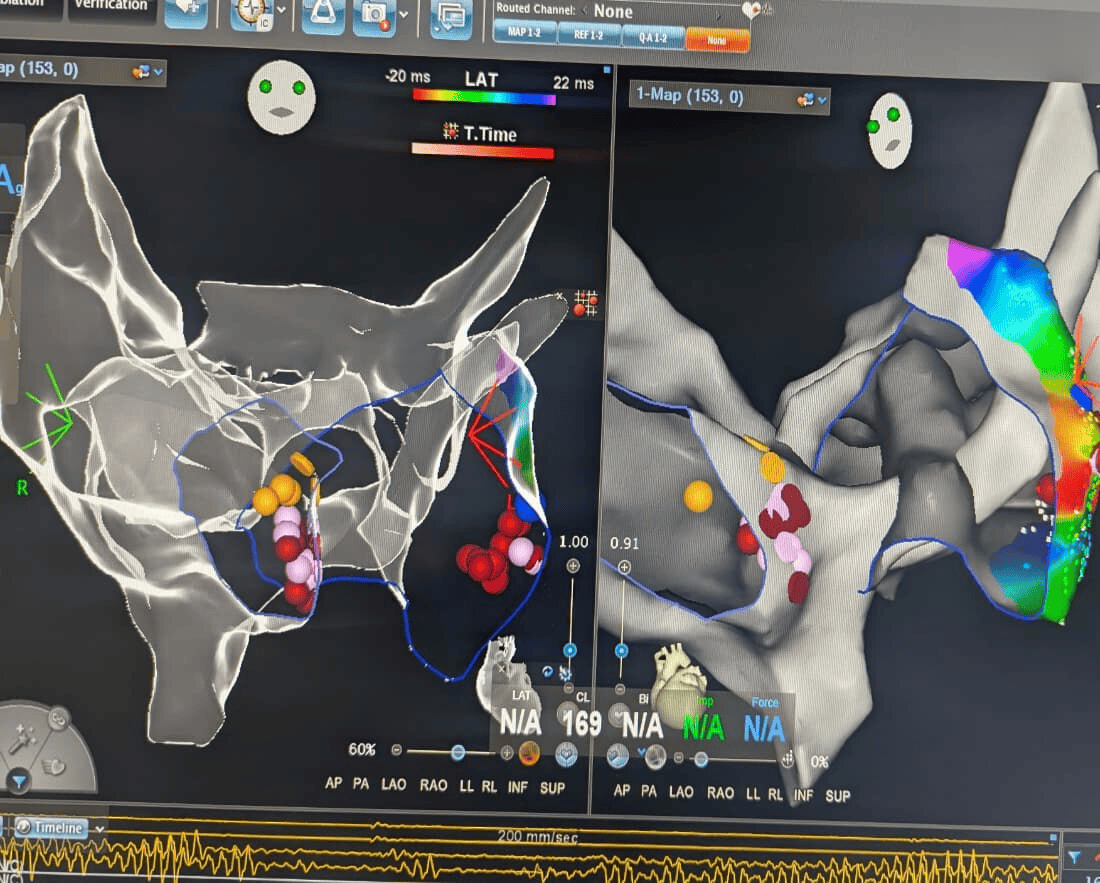
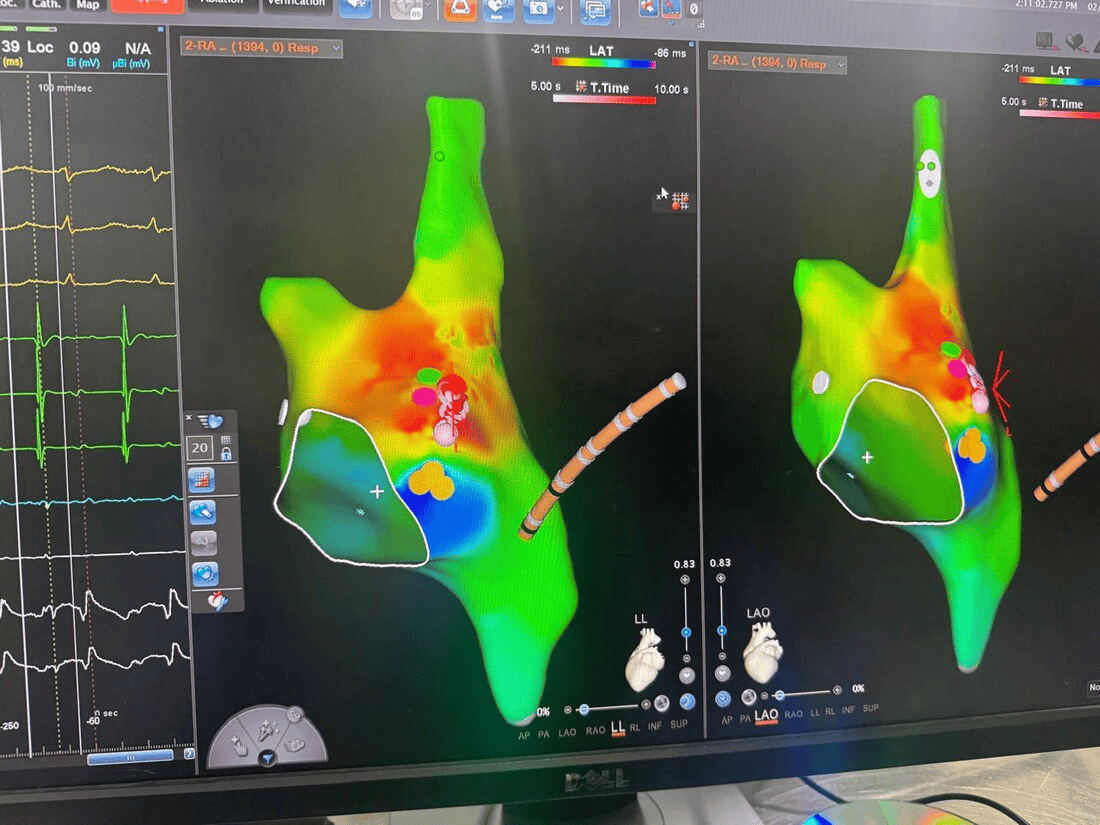
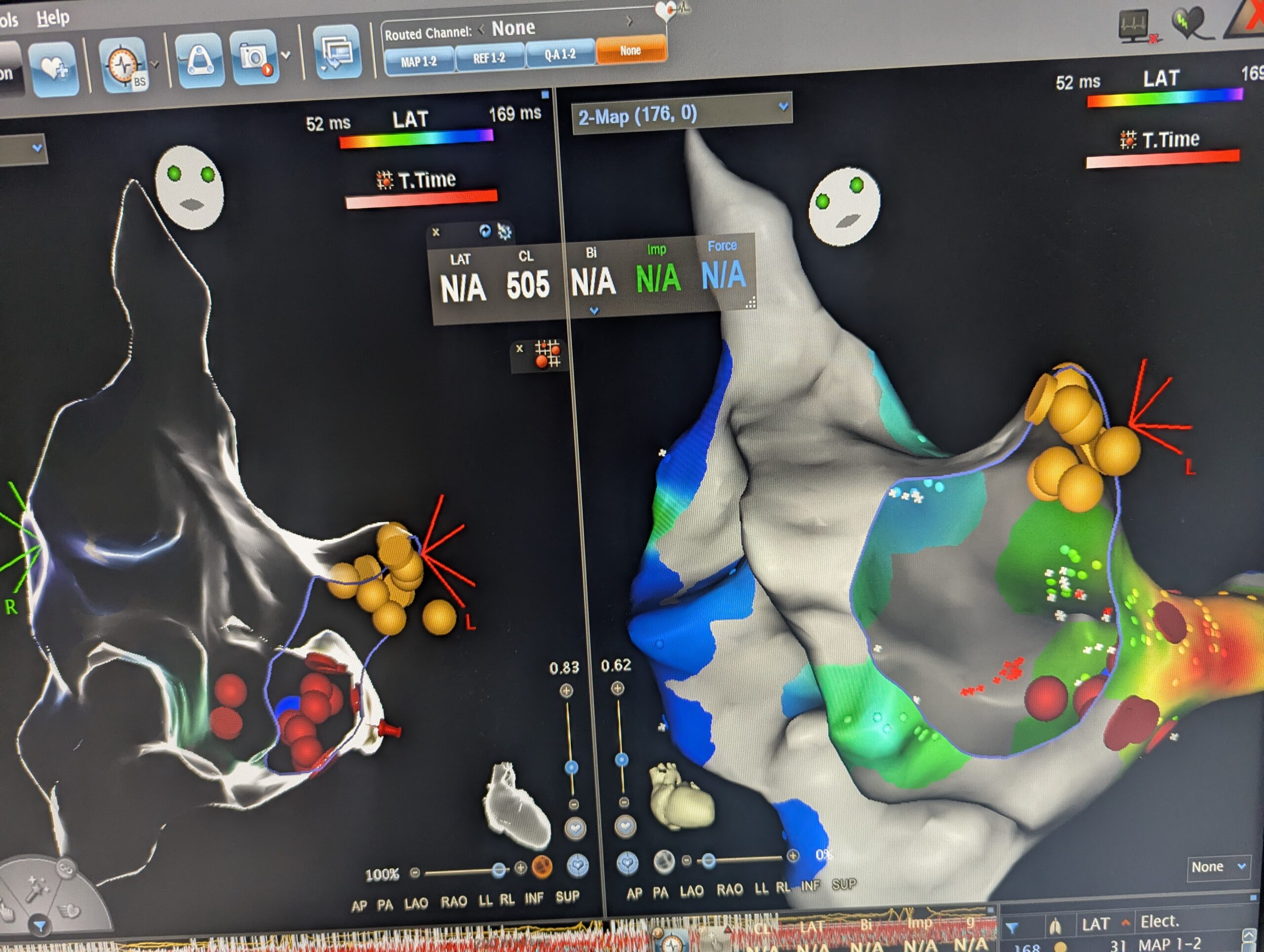
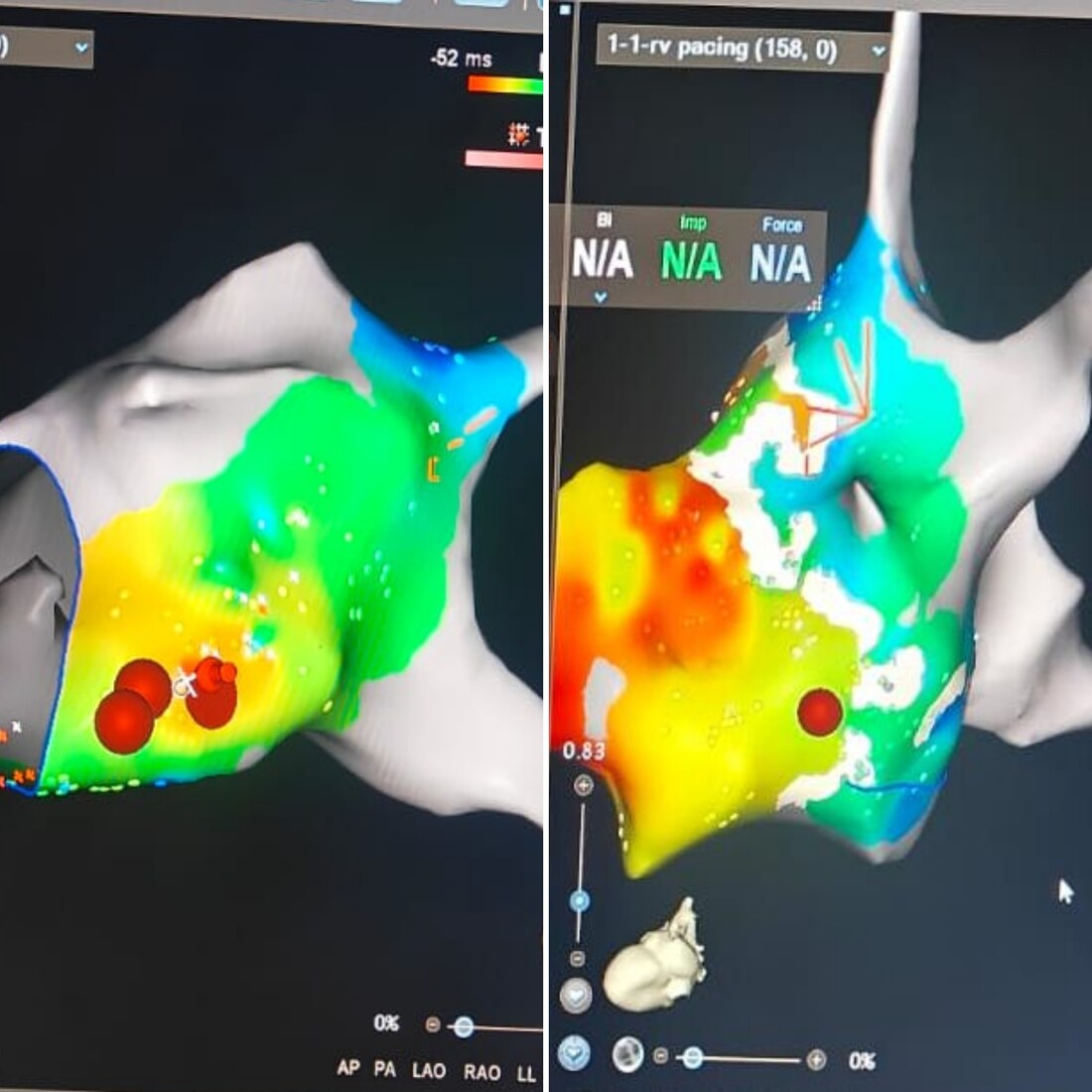
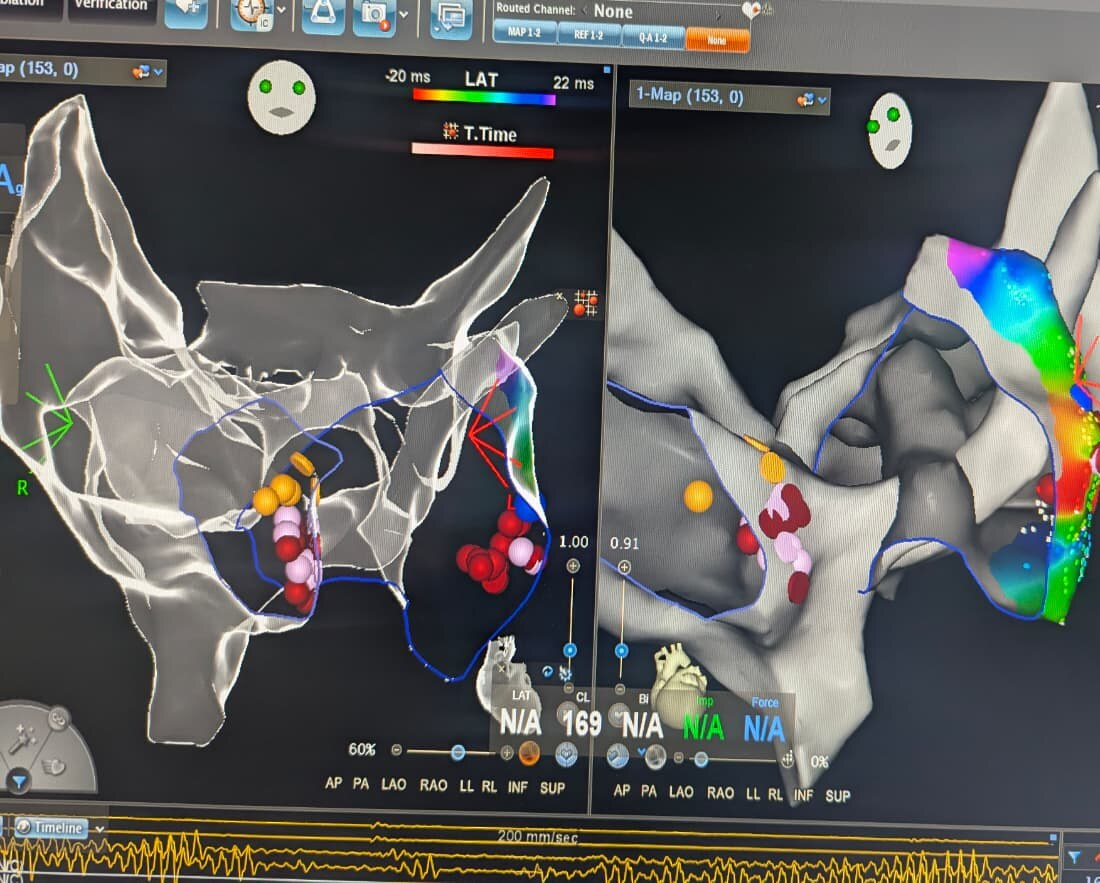
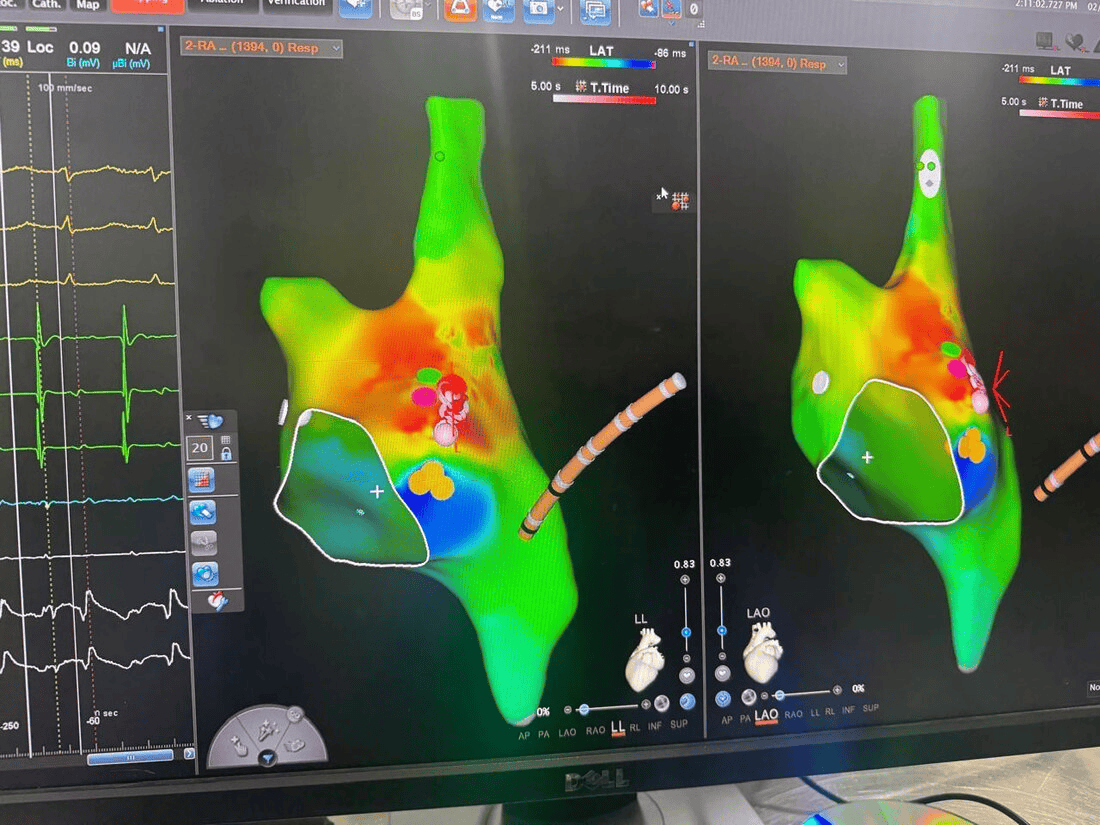
The Carto 3D maps below show two recent SVT ablations at HRHF Clinic — one on each side of the heart — both successfully eliminated.
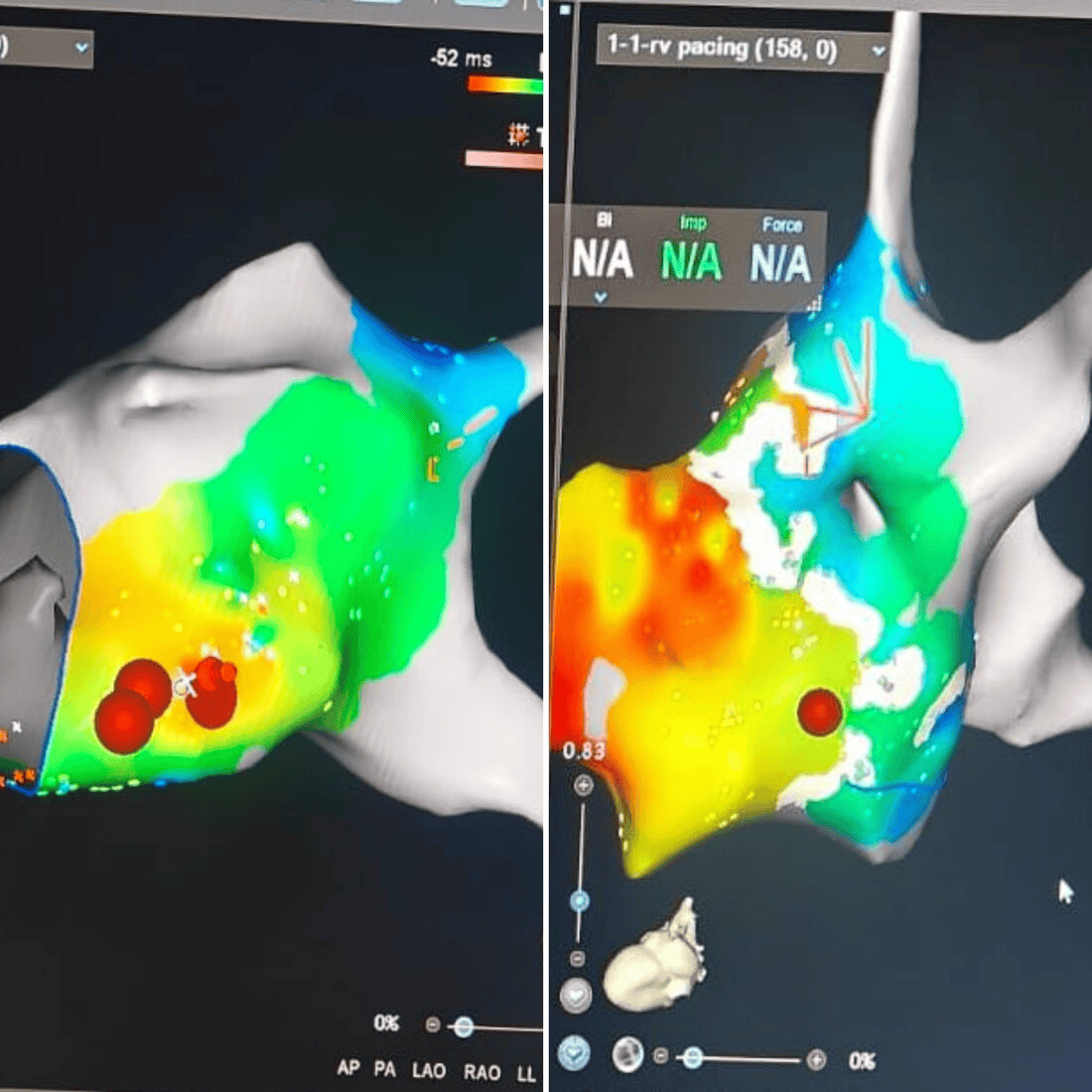
A concealed accessory pathway is one that conducts in only one direction — backwards from the ventricle to the atrium. It does not appear on a routine resting ECG. The pathway becomes evident only during an SVT episode, or when specifically searched for during an EP study. Identifying and ablating these pathways requires high-density 3D mapping with techniques such as open-window mapping during ventricular pacing.
When One Patient Has Two Different SVT Circuits — Both Ablated in a Single Procedure
In some patients, more than one arrhythmia mechanism is present simultaneously. This patient had both AVNRT — the most common form of SVT, arising from a re-entry circuit within the AV node itself — and a separate left lateral concealed accessory pathway creating a second, independent SVT circuit. Without comprehensive EP study and 3D mapping, one mechanism could easily be missed. Both were identified and ablated at HRHF Clinic in the same procedure.