
The Leadless Pacemaker — When the Right Pacemaker is No Pacemaker at All
A small capsule, placed entirely inside the heart through a vein in the leg. No chest scar. No generator pocket. No leads to fail. For the right patient, the leadless pacemaker is not just an alternative — it is the better answer.
National Medtronic Proctor for Micra
Dr. Rajesh Dhopeshwarkar is a Medtronic-certified national proctor for the Micra leadless pacemaker — one of a small number of physicians in India authorised to train and supervise other implanters. HRHF Clinic has implanted leadless pacemakers since the technology became available in India, with experience across the full spectrum of indications including the most challenging substrates.

Should I Choose a Leadless Pacemaker?
This is the most common question we are asked about leadless pacing — and the honest answer is: it depends on who you are. The leadless pacemaker is a transformative technology for the right patient and an unnecessary one for the wrong patient. Here is the framework we use in our consultations.
A leadless pacemaker is a small device — about the size of a large vitamin capsule — that is implanted directly inside the right ventricle through a catheter inserted in the femoral vein. No chest incision, no generator pocket, no leads to fail. This technology has fundamentally changed pacing in selected patient groups, but it is not the right answer for everyone. Conventional transvenous pacemakers remain appropriate for the majority, and the decision should be made based on clinical situation — not on novelty.
The Substrates Where Leadless is the Better Answer
In these specific clinical situations, leadless pacing is not merely an alternative — it is the safer, more durable choice. These are the patients we routinely advise toward leadless implantation.
-
Patients on Dialysis / Advanced CKD
End-stage renal disease, AV fistula, or advanced CKD — the leadless pacemaker eliminates pocket infection risk, preserves venous anatomy needed for dialysis access. First-line choice, not alternative.
-
Immunocompromised Patients
Post-transplant, biologics, chemotherapy — eliminating the pocket and leads removes the primary sites of pacemaker infection. Durable, infection-resistant solution.
-
Difficult / Compromised Vascular Access
Central venous occlusion, prior failed leads, congenital anomalies — femoral approach bypasses upper venous access entirely.
-
Previous Pacemaker Infection / Lead Extraction
High recurrence risk with transvenous device. Leadless pacemaker removes substrates that caused original infection.
-
Younger Active Patients
No visible chest bump, no arm restrictions, no recovery limitations. Ideal for athletes, swimmers, and professionals with aesthetic concerns.
-
Frail / Elderly with Thin Skin
Atrophic tissue, chest wall radiation, or erosion risk — leadless avoids pocket complications entirely.
When Leadless is NOT the Right Answer
Not appropriate for: patients requiring dual-chamber pacing where AV-synchronous pacing essential but Micra AV insufficient; extensive tricuspid valve disease; unfavourable femoral venous anatomy; severely dilated right ventricles. Decision after echocardiogram and venous evaluation.
Three Leadless Devices — Three Different Patients
Leadless pacing has evolved rapidly. There are now three distinct devices serving three distinct patient groups. Choosing the right one requires understanding what each is designed to do.
-
Micra VR (Medtronic)
The original single-chamber leadless pacemaker. Ventricular pacing for patients in atrial fibrillation with slow ventricular response, or those needing only intermittent pacing. Longest clinical experience.
-
Micra AV (Medtronic)
Accelerometer-based AV-synchronous pacing. Senses atrial mechanical activity, delivers synchronized ventricular pacing. For patients with AV block in sinus rhythm — the device that transformed leadless pacing into mainstream therapy.
-
Radiofrequency & Cryoablation
True dual-chamber leadless system: two devices (atrium + ventricle) that communicate wirelessly. For patients needing full dual-chamber pacing who cannot accept transvenous leads. HRHF Clinic offers Aveir DR as available in India.
Why Micra AV is the Workhorse
For most leadless candidates with intact sinus node function and AV block, Micra AV is the device of choice. The accelerometer-based atrial sensing achieves AV synchrony without a separate atrial lead — providing haemodynamic benefit in a single, contained device. For chronic AF with slow response, Micra VR remains ideal. For true dual-chamber needs, Aveir DR is the option.
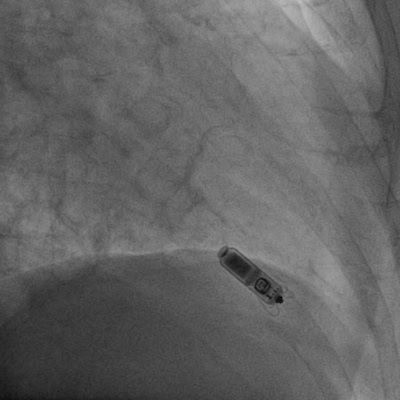
Case in Focus: Micra AV in a 70-Year-Old with Renal Dysfunction
A 70-year-old gentleman with significant renal dysfunction presented with high‑grade AV block and pre‑syncope. Conventional dual‑chamber transvenous pacing carried elevated risks — pocket infection in CKD, venous compromise interfering with future dialysis, and cumulative lead burden. Micra AV was the right answer.
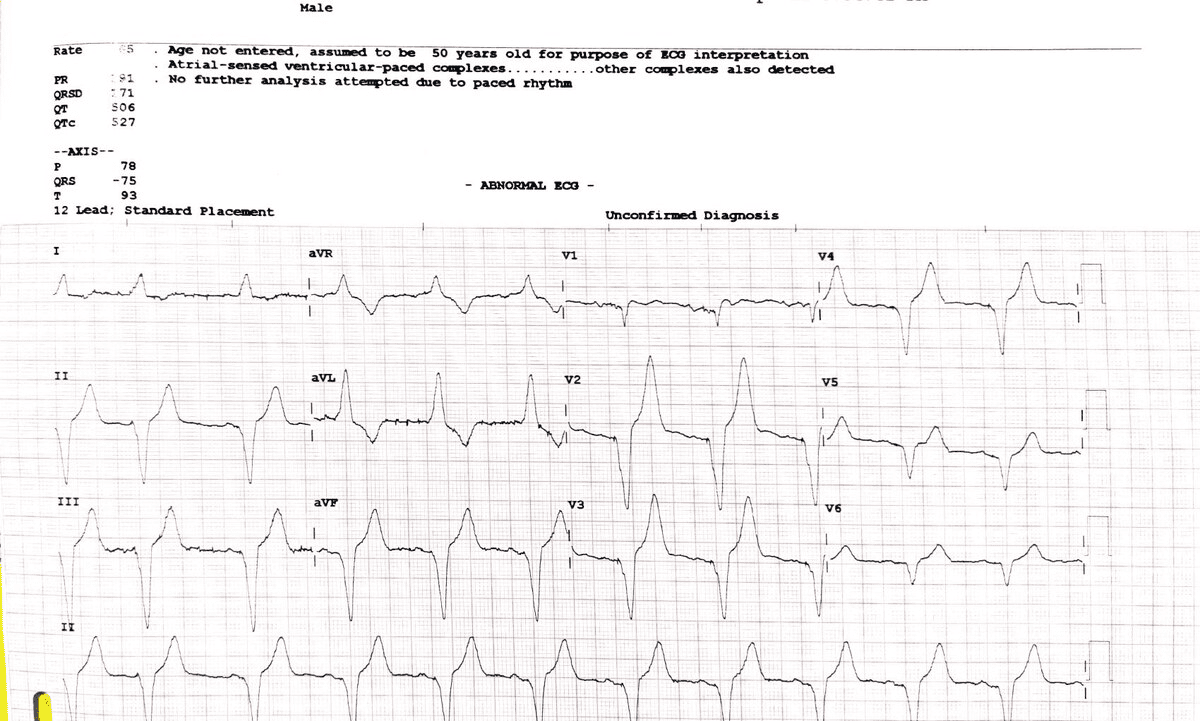
Outcome: Single device implanted through femoral vein, anchored at right ventricular apex, providing AV‑synchronous pacing via accelerometer‑based atrial sensing. No chest incision, no pocket, no subclavian access. Discharged within 24 hours.
POST-IMPLANT ECG
The Leadless Implant — From Admission to Discharge
-
Pre‑procedure
Echocardiogram, renal function, venous evaluation. Detailed counselling on device choice (VR/AV/DR). Anticoagulation review.
-
Day of procedure
Local anaesthesia + sedation. Femoral vein puncture → catheter to RV under fluoroscopy. Device deployed and tested. 30–60 min.
-
Recovery
Bed rest 3–4 hours, then mobilisation. Overnight monitoring. Discharge typically the next day.
-
Discharge
Typically the day after procedure. No chest sutures, no arm restrictions. Small groin puncture heals within days.
-
First Follow‑up
Two weeks after discharge: device interrogation, threshold testing, sensing parameters revie
-
Long-term
Routine follow-up at 3,6,12 months, then annually. Battery longevity ~10–12 years. End-of-life: second leadless device or transition.
Side by Side — How the Two Approaches Compare
| Aspect | Conventional Pacemaker | Leadless Pacemaker |
|---|---|---|
| Access route | Subclavian or cephalic vein (chest) | Femoral vein (groin) |
| Generator location | Pocket beneath chest skin | None — entire device inside heart |
| Visible scar | Yes, 4–5 cm chest scar | No chest scar (tiny groin puncture) |
| Leads in heart | 1–2 leads | No leads |
| Recovery time | 2–6 weeks, arm restrictions | 1–2 days, no chest restrictions |
| Pocket infection risk | Significant (CKD/immunocompromised) | Eliminated — no pocket |
| MRI compatibility | Conditional for modern devices | Fully MRI‑compatible |
| AV synchrony | Dual‑chamber lead system | Micra AV (accelerometer) or Aveir DR |
| Cost | Lower upfront | Higher upfront, offset by avoided complications in high‑risk groups |
Common Questions About Leadless Pacing
After ~10–12 years, a second leadless device can be implanted alongside the first; original is left encapsulated. Transition to transvenous may also be appropriate.
No. Nitinol tines anchor into heart muscle; tissue encapsulation occurs. Dislodgement rare in experienced hands.
Yes. All current leadless pacemakers (Micra, Aveir) are fully MRI‑compatible with appropriate programming.
No. Standard precautions as with all pacemakers; everyday electronics are safe.
Local anaesthesia + sedation. Femoral puncture is numbed; most patients find it much less discomfort than anticipated.
Favourable safety profile. Rare: cardiac perforation, pericardial effusion, femoral access issues, device dislodgement. Leadless eliminates pocket infection & lead failure.
Depends on indication. For intermittent pacing, infection risk, active lifestyle — excellent option. Detailed consultation required.
Higher upfront device cost. For high‑benefit groups (CKD, immunocompromised), cost offset by avoided infections, extractions, and admissions.
Referring Your Pacemaker Patient for Leadless Evaluation
HRHF Clinic accepts referrals for leadless pacemaker evaluation from across western India. Dr. Dhopeshwarkar is a Medtronic-certified national proctor for Micra and performs the procedure routinely at both centres. Many patients referred for conventional pacing turn out to be better leadless candidates.
-
Pacing in dialysis / advanced CKD
-
Immunocompromised patient
-
Previous pocket infection / extraction
-
Difficult or compromised upper venous access
-
Active lifestyle / aesthetic concerns
-
Frail elderly with thin chest tissue
-
Intermittent pacing needs in chronic AF (Micra VR)
-
Patient preference after thorough research
Find out if Leadless is the Right Pacemaker for You
An honest evaluation by a Medtronic national proctor — not a sales pitch. We will tell you whether leadless is the better choice for your specific situation, or whether conventional pacing is more appropriate.