
Bradycardia & Pacemakers — When Your Heart Beats Too Slowly
A slow heart rate is not always harmless. When bradycardia causes symptoms — or is severe enough to be dangerous — a pacemaker restores normal heart rhythm reliably and permanently. Modern pacing has evolved far beyond a simple device in the chest: today, pacing can be delivered with no chest scar, no visible device, or directly into the heart's own conduction system for a more natural rhythm.
HRHF Clinic — Western Maharashtra's Highest Volume Conduction System Pacing Programme
Dr. Rajesh Dhopeshwarkar performs His bundle pacing, Left Bundle Branch Area Pacing, and Bachmann Bundle Pacing routinely — the full spectrum of physiological pacing. He is a Medtronic-certified national proctor for the Micra leadless pacemaker and CRT devices. HRHF Clinic has the highest conduction system pacing volume in western Maharashtra.
HBP
His Bundle Pacing
LBBAP
Left Bundle Area
BBP
Bachmann Bundle
Micra
Leadless Pacing
CRT
Resynchronisation
A Heart That Beats Too Slowly
The normal resting heart rate is 60 to 100 beats per minute. Bradycardia simply means a heart rate below 60 bpm. In many people — particularly fit individuals and athletes — a slow heart rate is entirely normal and not a concern. But when a slow heart rate causes symptoms, or when it falls dangerously low due to a problem with the heart's electrical system, it requires evaluation and often treatment.
Common Symptoms
- Dizziness or light-headedness
- Fainting or near-fainting (syncope)
- Unexplained fatigue and reduced exercise tolerance
- Breathlessness on mild exertion
- Confusion or cognitive slowing (elderly)
- Some patients have no symptoms — found incidentally
Common Causes
- Sick Sinus Syndrome — sinus node disease
- AV block — 1st, 2nd (Mobitz I/II), 3rd degree
- Congenital heart block
- Post-cardiac surgery conduction damage
- Medications — beta-blockers, calcium channel blockers, digoxin
- Age-related degeneration of conduction tissue
Not All Pacemakers Are the Same
The right pacemaker depends on the indication, the underlying anatomy, and the patient's specific clinical needs. HRHF Clinic offers the full spectrum — from conventional single and dual chamber devices to the most advanced physiological pacing techniques available.
| Pacing Type | What it does | Best for |
|---|---|---|
| Single chamber (VVI/AAI) | One lead in the right ventricle or right atrium. Paces the chamber when the rate drops below the programmed limit. | Chronic AF with slow ventricular rate. Intermittent AV block with intact sinus node. |
| Dual chamber (DDD) | Two leads — one in the right atrium, one in the right ventricle. Coordinates AV timing to preserve the natural atrial contribution to cardiac output. | AV block in sinus rhythm. Sick Sinus Syndrome. Most patients requiring permanent pacing. |
| CRT-P / CRT-D | Adds a third lead to the left ventricle via the coronary sinus. Resynchronises both ventricles for heart failure patients with wide QRS. | Heart failure with LBBB and reduced EF. Pacing-induced cardiomyopathy. |
| His Bundle Pacing (HBP) | Paces the His bundle — the main electrical highway — producing a narrow, synchronous QRS. First form of true conduction system pacing. | AV block with preserved His-Purkinje. Pacing-induced cardiomyopathy. CRT alternative. |
| Left Bundle Branch Area Pacing (LBBAP) | Deep septal lead deployment capturing the left bundle branch or its fascicles. Narrow QRS, true physiological pacing. More reliable than HBP. | AV block — especially congenital CHB. Young patients requiring long-term pacing. CRT non-responders. |
| Bachmann Bundle Pacing (BBP) | Paces at the interatrial conduction bridge — restoring normal right-to-left atrial activation. Reduces interatrial conduction delay and AF risk. | SSS with wide notched P wave. LVH with diastolic dysfunction. Patients where interatrial delay drives AF. |
| Leadless Pacing (Micra) | Entire device inside the right ventricle. No chest pocket, no leads, no scar. | CKD / dialysis. Immunocompromised. Previous pocket infection. Active lifestyle. |
Single and Dual Chamber Pacemakers
Conventional pacemakers have been transforming lives since the 1960s. A small generator — placed in a pocket beneath the skin below the collarbone — connects via one or two leads threaded through a vein to the chambers of the heart. When the heart rate drops below the programmed limit, the device delivers a small electrical impulse to restore rhythm.
Single chamber pacemakers place one lead in the right ventricle (VVI) or right atrium (AAI). Dual chamber devices add a second lead so that both chambers work in synchrony, preserving the natural AV timing that contributes to cardiac output. For most patients requiring permanent pacing — AV block, sick sinus syndrome — a dual chamber system is the standard approach.
Conventional pacing works reliably and durably. The limitation is the site of ventricular pacing: stimulating the right ventricle from the apex produces an abnormal, wide QRS pattern — electrical dyssynchrony that, over years, can lead to progressive left ventricular dysfunction in a significant proportion of patients. This is the problem that conduction system pacing was designed to solve.

Left Bundle Branch Area Pacing — LBBAP
The Principle
Conduction system pacing delivers the pacing impulse directly to the heart's own electrical highway — the His bundle or the left bundle branch — rather than to the working myocardium. The result is a narrow, synchronous QRS that looks and behaves like normal ventricular activation. It is not an approximation of physiological pacing — it is physiological pacing.
Left Bundle Branch Area Pacing is now the preferred form of CSP at HRHF Clinic. The pacing lead is screwed deep into the interventricular septum until it captures the left bundle branch or its proximal fascicles. The electrical result — confirmed by RBBB morphology in V1 with a narrow QRS — is synchronous biventricular activation via the intact His-Purkinje system. For a young patient requiring decades of pacing, this difference compounds into a clinically meaningful preservation of left ventricular function.
Indications for LBBAP
- Any patient requiring permanent ventricular pacing who is young or active — physiological pacing from the outset prevents future pacing-induced cardiomyopathy
- Congenital complete heart block — the block is typically at the AV node, LBBAP bypasses it while preserving the entire distal conduction system
- Pacing-induced cardiomyopathy — upgrade from conventional RV pacing to LBBAP in patients with declining LV function
- CRT non-responders — LBBAP achieves true left-sided conduction system recruitment where CRT cannot
- AV block with intact His-Purkinje — where HBP threshold is prohibitively high, LBBAP achieves the same physiological result with better lead stability and lower thresholds
| Conventional RV Pacing | LBBAP |
|---|---|
| Broad LBBB-pattern QRS — electrical dyssynchrony | Narrow QRS — synchronous biventricular activation |
| Unphysiological activation sequence | His-Purkinje system recruited — normal activation |
| Pacing-induced cardiomyopathy in up to 20% long-term | LV function preserved long-term |
| RV apex stimulation causes septal remodelling | Septal activation normal — no remodelling |
| CRT needed if LV function declines | CRT rarely needed — physiological from the start |
-
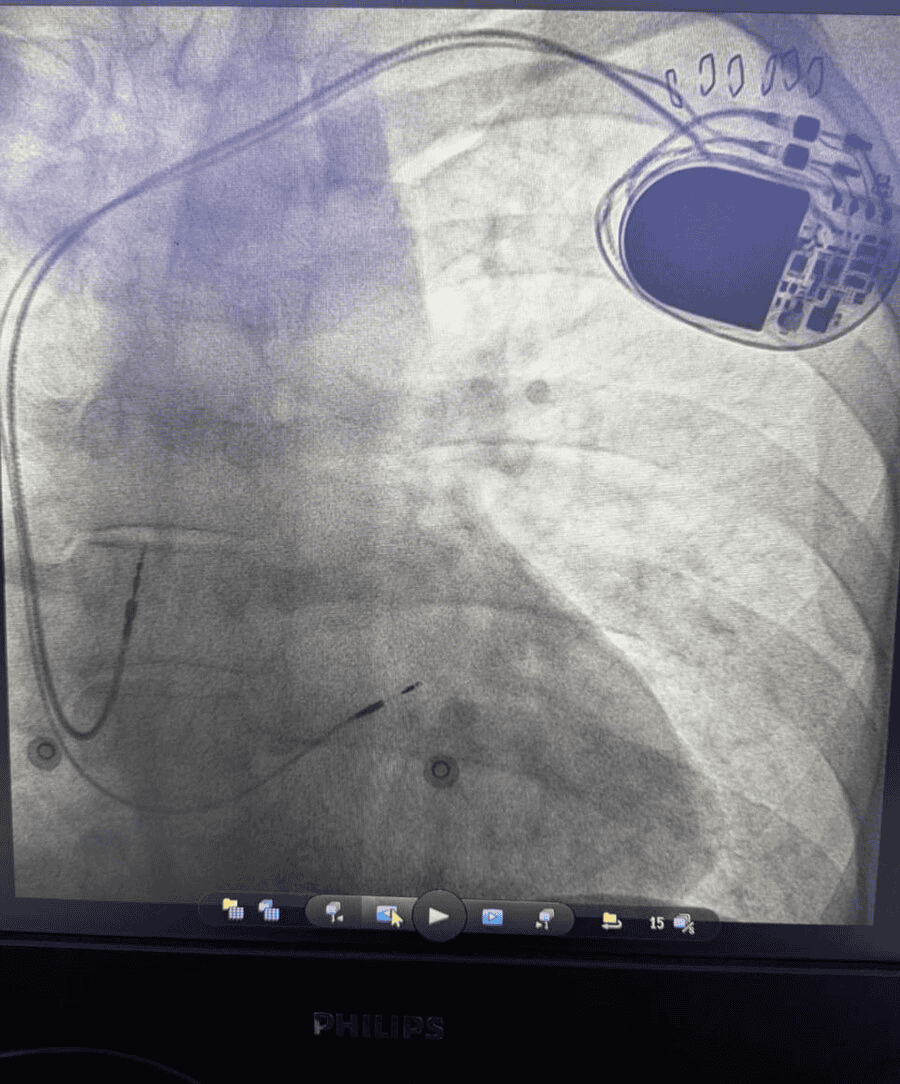
LBBAP Case — 36-Year-Old with Congenital Complete Heart Block
A 36-year-old with congenital CHB and a structurally normal heart faces potentially 40 to 50 years of pacing. Conventional RV apical pacing would subject this patient to decades of electrical dyssynchrony and the cumulative risk of pacing-induced cardiomyopathy. LBBAP was performed at HRHF Clinic — delivering a narrow paced QRS by recruiting the left bundle branch distal to the AV block site. Long-term LV function is preserved and the physiological activation sequence restored from day one.
Bachmann Bundle Pacing — Physiological Atrial Pacing
The Principle
While conduction system pacing is usually discussed in the context of ventricular activation, the atrial side matters too. The Bachmann bundle is the main interatrial muscle bridge — the normal route by which electrical activation travels from the right atrium to the left atrium. When this pathway is diseased or conducting slowly, the result is a wide, notched P wave on the ECG — interatrial conduction delay — which predisposes to atrial fibrillation and worsens haemodynamics.
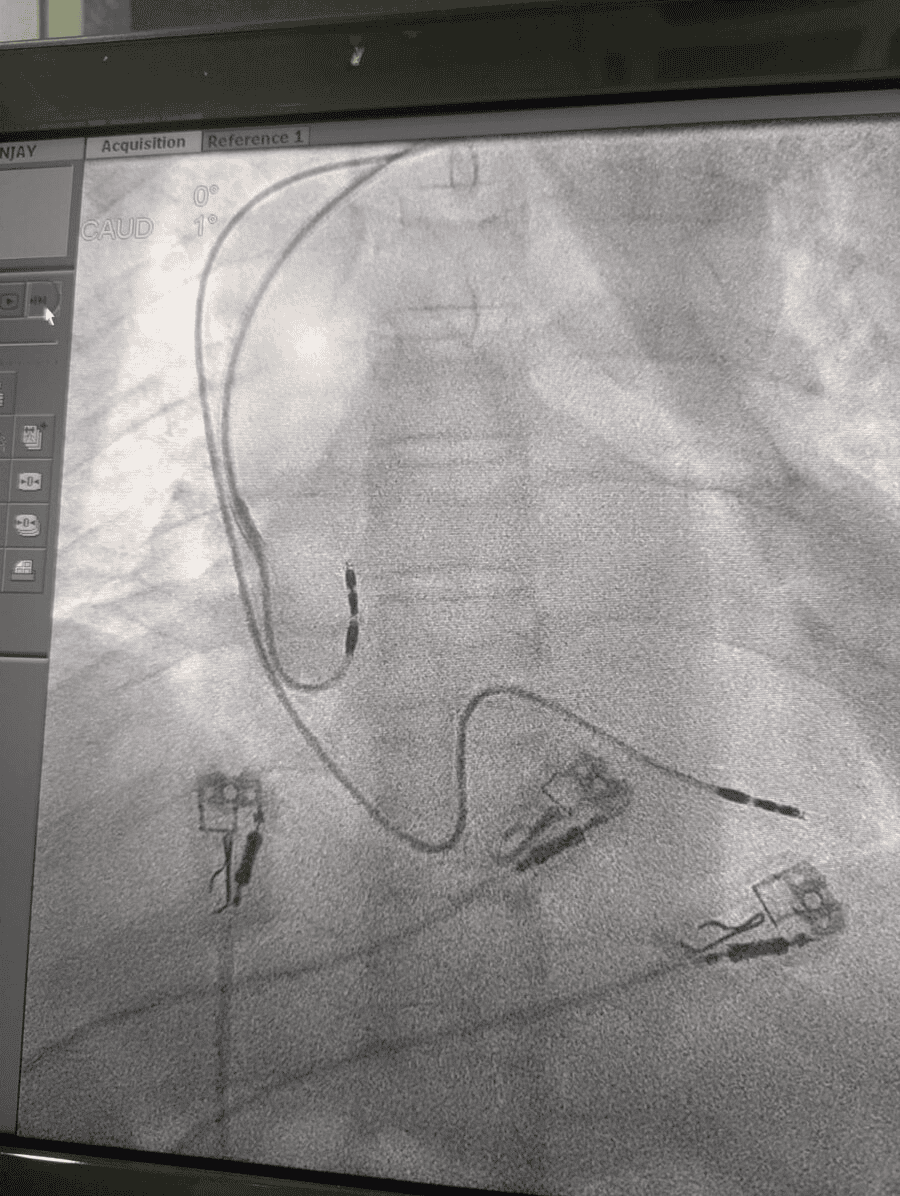
Conventional right atrial appendage (RAA) pacing may worsen interatrial delay because the stimulation site is remote from the Bachmann bundle. Pacing directly at the Bachmann bundle — at the superior interatrial septum — restores the normal right-to-left atrial activation sequence, shortens the paced P wave duration, and may reduce AF burden in susceptible patients.
HRHF Clinic performs Bachmann bundle pacing routinely — one of very few centres in western India with established experience in this technique.
When to Choose BBP Over Conventional RAA Pacing
- Sick Sinus Syndrome with wide notched P wave (>120ms) — interatrial delay identified on baseline ECG
- LVH with diastolic dysfunction — substrate where atrial dyssynchrony from conventional pacing is particularly harmful
- Paroxysmal AF driven by interatrial conduction delay — BBP as rhythm control strategy
- Patients with a history of AF who require pacing — BBP to reduce recurrence risk
-
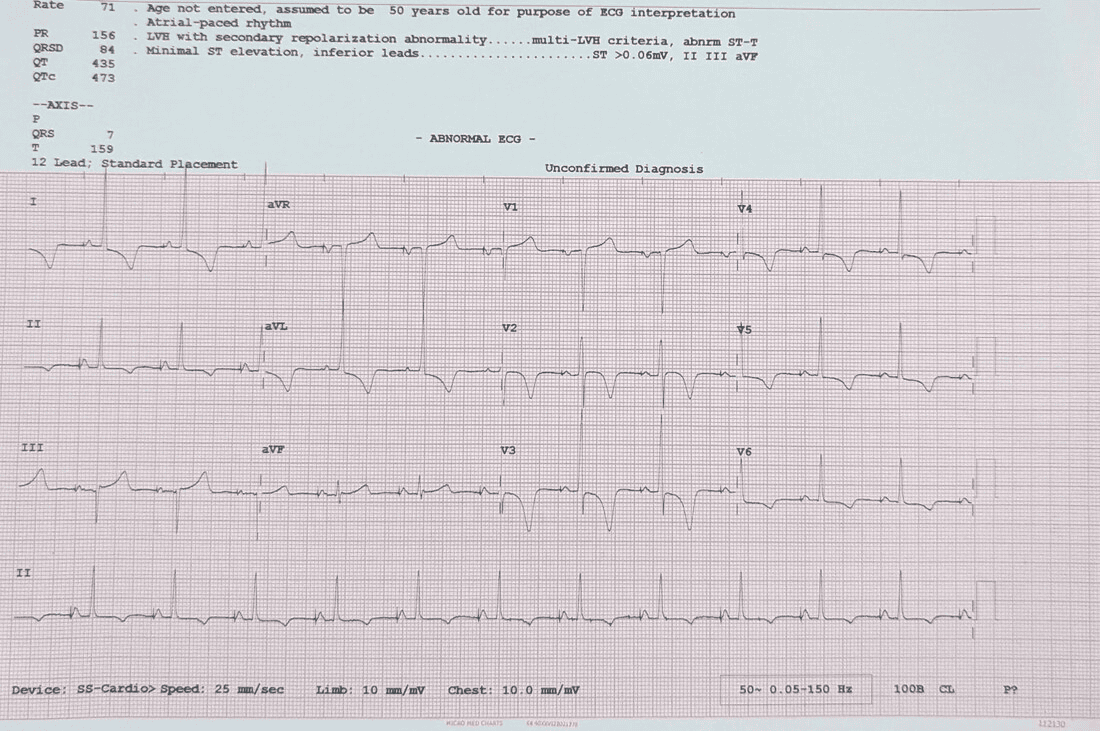
The Key Measurable — P Wave Duration
Successful Bachmann bundle capture is confirmed by measurable P wave shortening on the post-implant ECG. In our experience, P wave duration reduces from a baseline of 130–150ms to 85–100ms after BB capture — a 30 to 40 percent reduction in interatrial conduction time. If the P wave does not shorten, BB capture has not been achieved and the lead position requires adjustment.
-
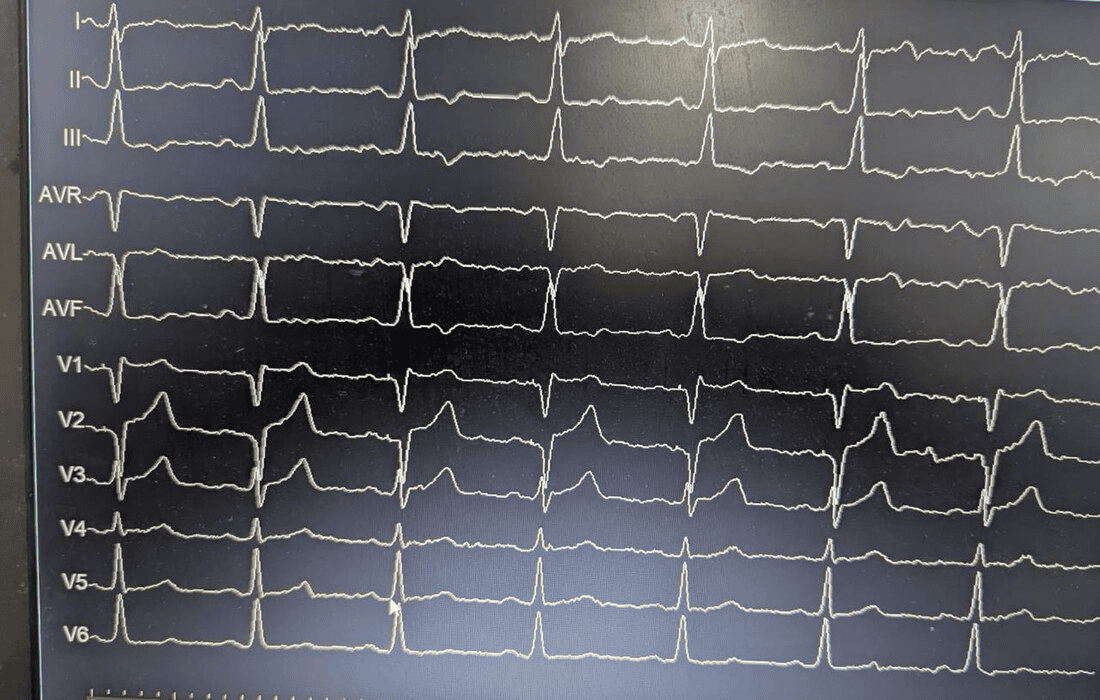
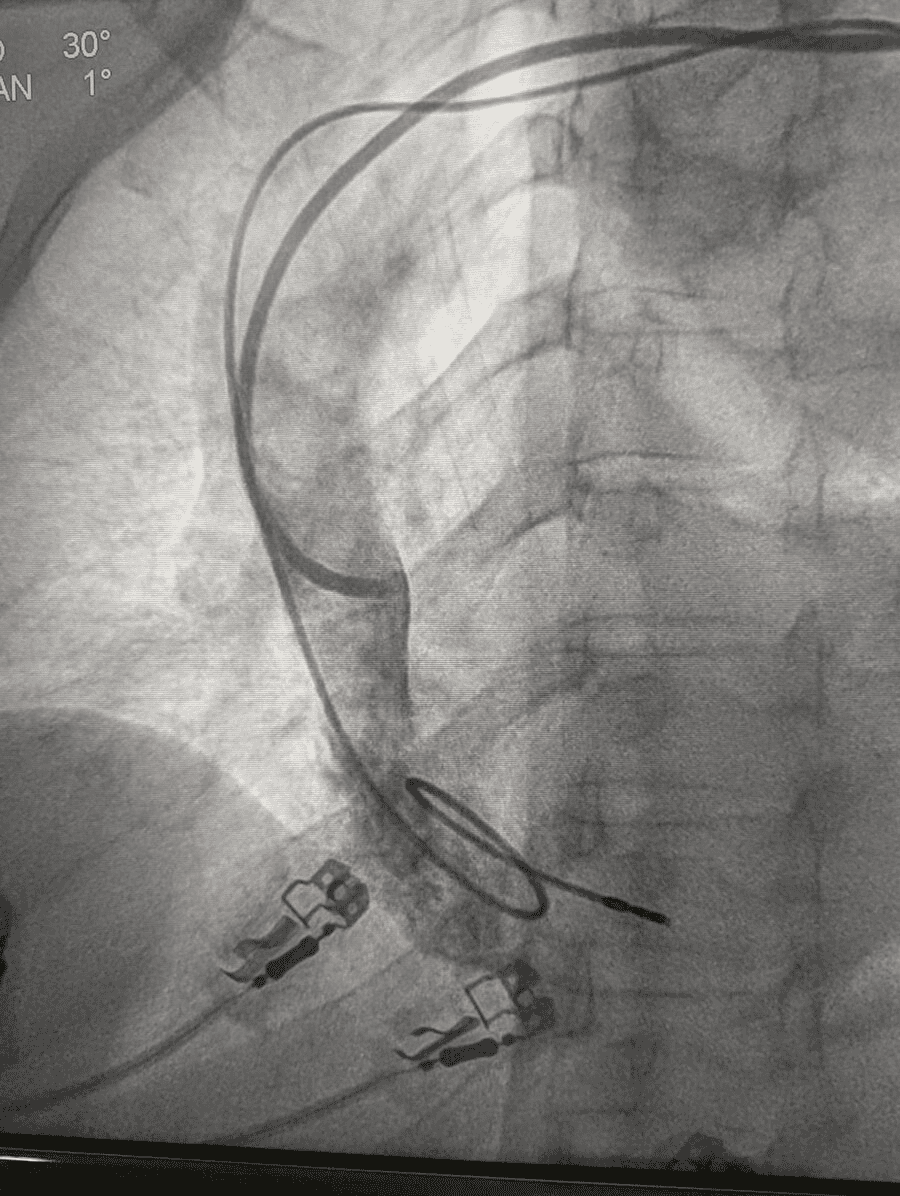
BBP Case — P Wave 130ms → 85ms
Sick Sinus Syndrome with Interatrial Conduction Delay
A 60-year-old male with hypertension, hypothyroidism, and single functioning kidney presented with symptomatic SSS — pauses to 3.1 seconds on Holter, minimum HR 30 bpm. Baseline 12-lead ECG showed a wide notched P wave of 130ms — significant interatrial conduction delay in the context of concentric LVH and Grade I diastolic dysfunction. Conventional RAA pacing would worsen this delay and increase AF risk. Bachmann bundle pacing was performed — confirmed by P wave reduction from 130ms to 85ms on the post-implant ECG, confirming successful BB capture and restoration of synchronous biatrial activation.
Which Conduction System Pacing Approach — A Quick Reference
For referring physicians and patients, here is a quick reference guide for matching the clinical scenario to the most appropriate pacing strategy at HRHF Clinic.
| Clinical Scenario | Preferred Approach | Rationale |
|---|---|---|
| Young patient, AV block, structurally normal heart | LBBAP | Decades of pacing ahead — physiological from day one prevents future cardiomyopathy |
| SSS + wide P wave + LVH/diastolic dysfunction | Bachmann Bundle Pacing | Interatrial delay identified — RAA pacing would worsen it; BBP restores normal biatrial activation |
| AV block + declining LV on existing RV pacing | Upgrade to LBBAP | Pacing-induced cardiomyopathy — LBBAP achieves narrow QRS and restores LV function without CRT |
| CRT non-responder with AF | LBBAP | True left bundle recruitment where biventricular pacing cannot achieve adequate resynchronisation |
| High-degree AV block + AF (no sinus rhythm) | Dual chamber or LBBAP | AV synchrony not required if AF present; LBBAP for narrow QRS; dual chamber if sinus rhythm restores |
| Dialysis patient / CKD / previous infection | Leadless (Micra) | Eliminating pocket and leads eliminates the source of infection risk |
| Heart failure + LBBB + EF <35% | CRT-P or CRT-D | Primary CRT indication; LBBAP as alternative if CS lead cannot be placed or CRT non-response |
The Procedure — From Admission to Discharge
| Stage | What happens |
|---|---|
| Pre-procedure | Echocardiogram, blood tests, ECG. Review of pacing indication and optimal device choice — which pacing strategy is right for this specific patient. Medication review. |
| Day of procedure | Admission in the morning. Local anaesthesia and sedation. Lead(s) placed through the subclavian or cephalic vein; generator in the chest pocket for conventional pacing. For LBBAP and BBP, additional fluoroscopy time is required for precise lead placement — typically 1 to 2 hours total. |
| Recovery | Monitoring overnight. Wound check. Pacing threshold and sensing parameters confirmed on the programmer before discharge. |
| Discharge | Typically the day after the procedure. Arm restrictions on the implant side for 2 to 4 weeks — no lifting above the shoulder, no strenuous upper body activity. Wound care instructions. |
| First follow-up | Two weeks — wound check and device interrogation. Then at 3 months, 6 months, and annually thereafter. |
| Long-term | Pacemaker battery lasts 8 to 12 years typically. Routine annual checks monitor battery status and lead performance. When battery depletes — generator change (leads reused). Follow-up is lifelong but usually straightforward. |
Referring Your SVT Patient
SVT ablation is a high-volume procedure at HRHF Clinic. Dr. Dhopeshwarkar performs catheter ablation for AVNRT, AVRT, WPW, atrial tachycardia, and atrial flutter routinely, with over fifteen years of experience. Same working day acknowledgement of all referrals. Direct access for pre-referral discussion.
We particularly welcome referrals of: young patients with documented SVT who would benefit from cure rather than continued medical management; patients with WPW; patients in whom prior ablation has failed; and patients in whom medical therapy is poorly tolerated.
-
Direct Referral Contact
Phone: +91 96571 38400
Email: cardiologypune@gmail.com
Full referral pathway: Referring Doctors page →
Common Questions About Pacemakers
Most patients do not feel the pacing impulses at all. You may notice that your heart rate feels more regular and your energy improves. The generator may be visible as a small lump under the skin — this is normal and gradually becomes less noticeable as swelling settles.
Yes. Modern pacemakers are not significantly affected by mobile phones, microwaves, induction cookers, or airport security gates. Standard precautions about strong industrial magnets and MRI (see below) apply.
Most modern pacemakers — including all devices implanted at HRHF Clinic — are MRI-conditional. This means you can have an MRI with appropriate device programming before and after. Always carry your pacemaker card when attending for any MRI.
Typically 8 to 12 years depending on how much pacing the device delivers. When the battery approaches depletion, a generator change is performed — a much smaller procedure than the original implant, as the leads are reused.
After the initial 4 to 6 week healing period, most patients can return to all normal activities. There are no long-term exercise restrictions for pacemaker patients in most cases. Swimming, gym, yoga, and travel are all fine. Specific restrictions — if any — will be discussed at your follow-up.
Modern pacemakers are extremely reliable. They have multiple backup functions built in. If you notice your heart racing or feel faint, seek medical attention — your pacemaker clinic can interrogate the device within minutes to check its function. Carry your pacemaker card and emergency contact details at all times.
A pacemaker reliably prevents your heart from going too slowly. It does not cure the underlying cause of the bradycardia — the sinus node disease or AV block that made the pacemaker necessary. But it ensures your heart rate is always supported at a safe level, eliminating the symptoms of bradycardia.
Not all pacemakers are the same. Neither is the expertise behind them.
From conventional dual-chamber pacing to left bundle branch pacing, Bachmann bundle pacing, and leadless implantation — HRHF Clinic offers western Maharashtra's most complete pacing programme, in the hands of a Medtronic-certified national proctor.