
Atrial Fibrillation Ablation at HRHF Clinic
Western India's largest AF ablation programme — RF ablation with vHPSD and QDot technology, Cryoablation, and Pulsed Field Ablation. Every modality. One centre. One specialist.
Largest series of AF ablation procedures in western India
Dr. Dhopeshwarkar has been performing AF ablation for over fifteen years — with volume and outcomes that place this programme among the leading independent EP centres in the country.
Understanding Atrial Fibrillation
Atrial fibrillation — AF — is the most common sustained heart rhythm disorder. In AF, the upper chambers of the heart fire electrical signals chaotically instead of in a coordinated rhythm. The result is an irregular, often fast heartbeat that the patient feels as palpitations, breathlessness, fatigue, or dizziness. AF is not merely a nuisance. Untreated AF significantly increases the risk of stroke — because the chaotic rhythm allows blood to pool and clot in the heart. It also causes progressive deterioration of heart function over time, particularly if the heart rate remains poorly controlled.
Common AF Symptoms
-
Palpitations — irregular, rapid heartbeat
-
Breathlessness on exertion or at rest
-
Fatigue and reduced exercise tolerance
-
Dizziness or light-headedness
-
Chest discomfort or pressure
-
Some patients have no symptoms at all
Why AF Matters
-
5× increased risk of stroke
-
Progressive deterioration of heart function
-
Risk of heart failure with long-term uncontrolled AF
-
Dizziness or light-headedness
-
Reduced quality of life and exercise capacity
-
Cognitive decline — emerging evidence
The good news is that AF is treatable — and in the right patient, catheter ablation offers the best chance of restoring and maintaining normal rhythm for the long term.
Medicines vs Ablation — What is the Difference?
Medicines for AF fall into two categories — rate control, which slows the heart down without addressing the rhythm; and rhythm control, which attempts to maintain sinus rhythm using anti-arrhythmic drugs. Both have limitations. Rate control medicines do not restore normal rhythm. Rhythm control medicines are moderately effective but carry side effects, and they do not work well long term for many patients.
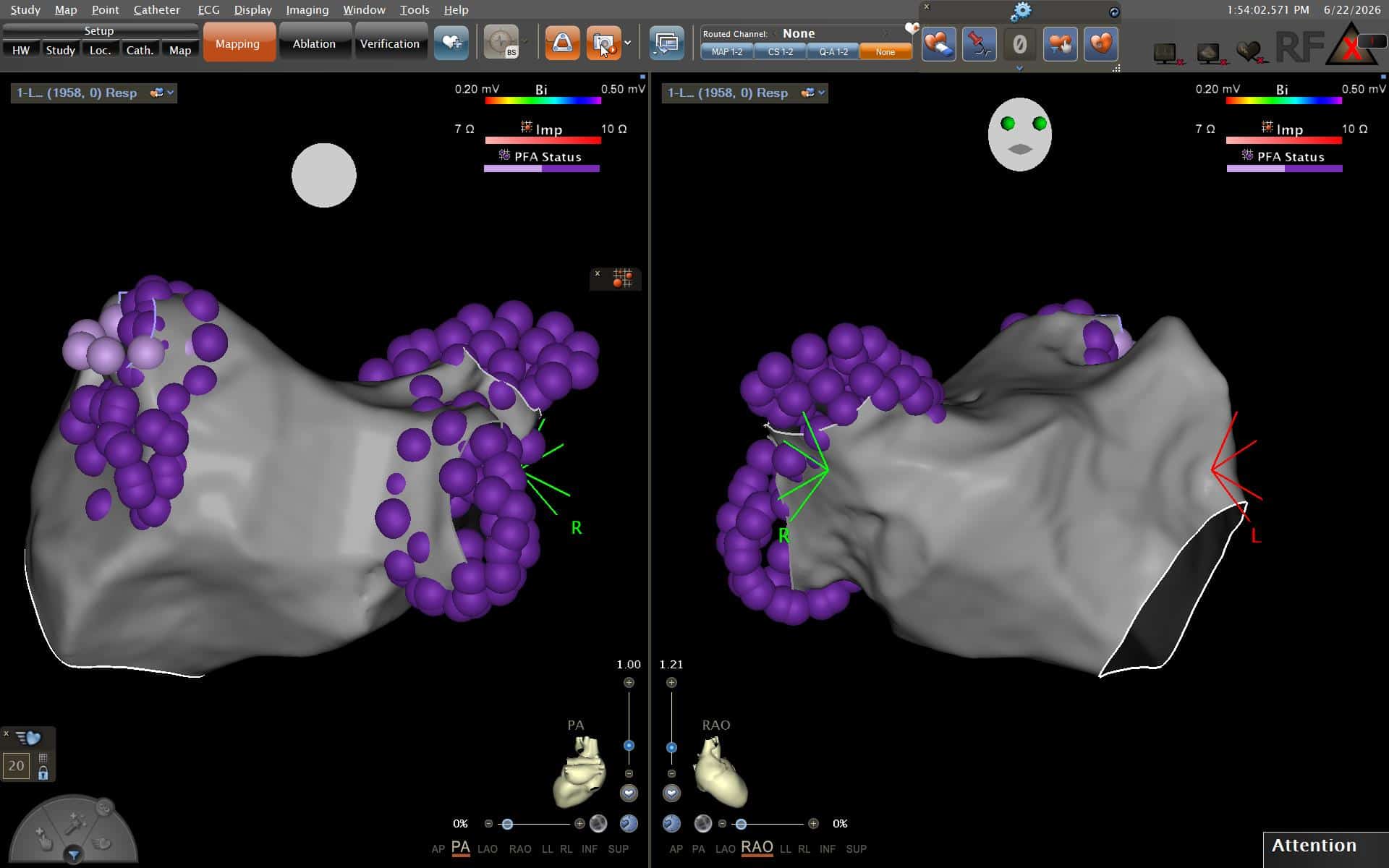
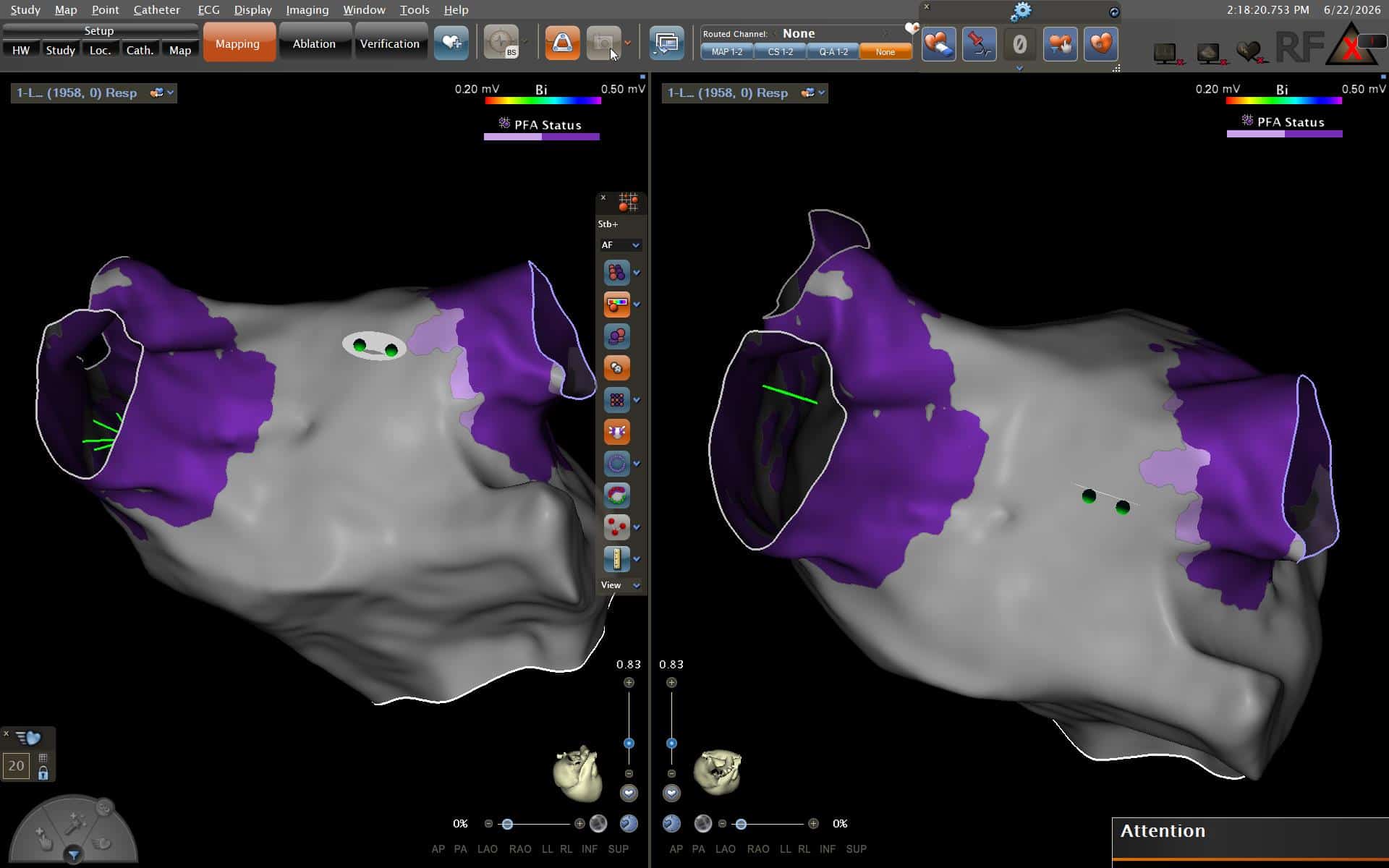
Catheter ablation addresses the cause of AF directly. The triggers for AF in most patients arise from electrical signals firing abnormally from the pulmonary veins — the four veins that connect the lungs to the left atrium. Ablation electrically isolates these veins from the rest of the atrium, eliminating the source of the abnormal signals. This is called pulmonary vein isolation (PVI).
Three Technologies. One Programme. The Right Choice for Each Patient.
HRHF Clinic offers the complete range of AF ablation modalities — RF ablation using vHPSD with QDot, Cryoablation, and Pulsed Field Ablation. No single technology is right for every patient. The choice is made based on AF type, anatomy, prior procedures, and individual clinical factors.
-
RF Ablation — vHPSD with QDot
Primary modality
Very high power short duration (90W/4s) with Thermocool SmartTouch QDot catheter. Contact force + temp-controlled delivery for precise, consistent lesions. Standard approach for majority of AF ablation procedures.
-
Cryoablation
First-line for paroxysmal AF
Freezing energy using Arctic Front Advance cryoballoon. Excellent for paroxysmal AF with consistent circumferential isolation, favourable safety profile, and strong long-term outcomes. Selected for appropriate patients as a first-line option.
-
Pulsed Field Ablation
Launched- NM Wadia Centre
Non-thermal, tissue-selective energy delivery. Spares adjacent structures (oesophagus, phrenic nerve). The most significant advance in AF ablation in a decade. HRHF Clinic is establishing PFA capability at NM Wadia Institute of Cardiology.
Very High Power Short Duration RF Ablation — What It Means for You
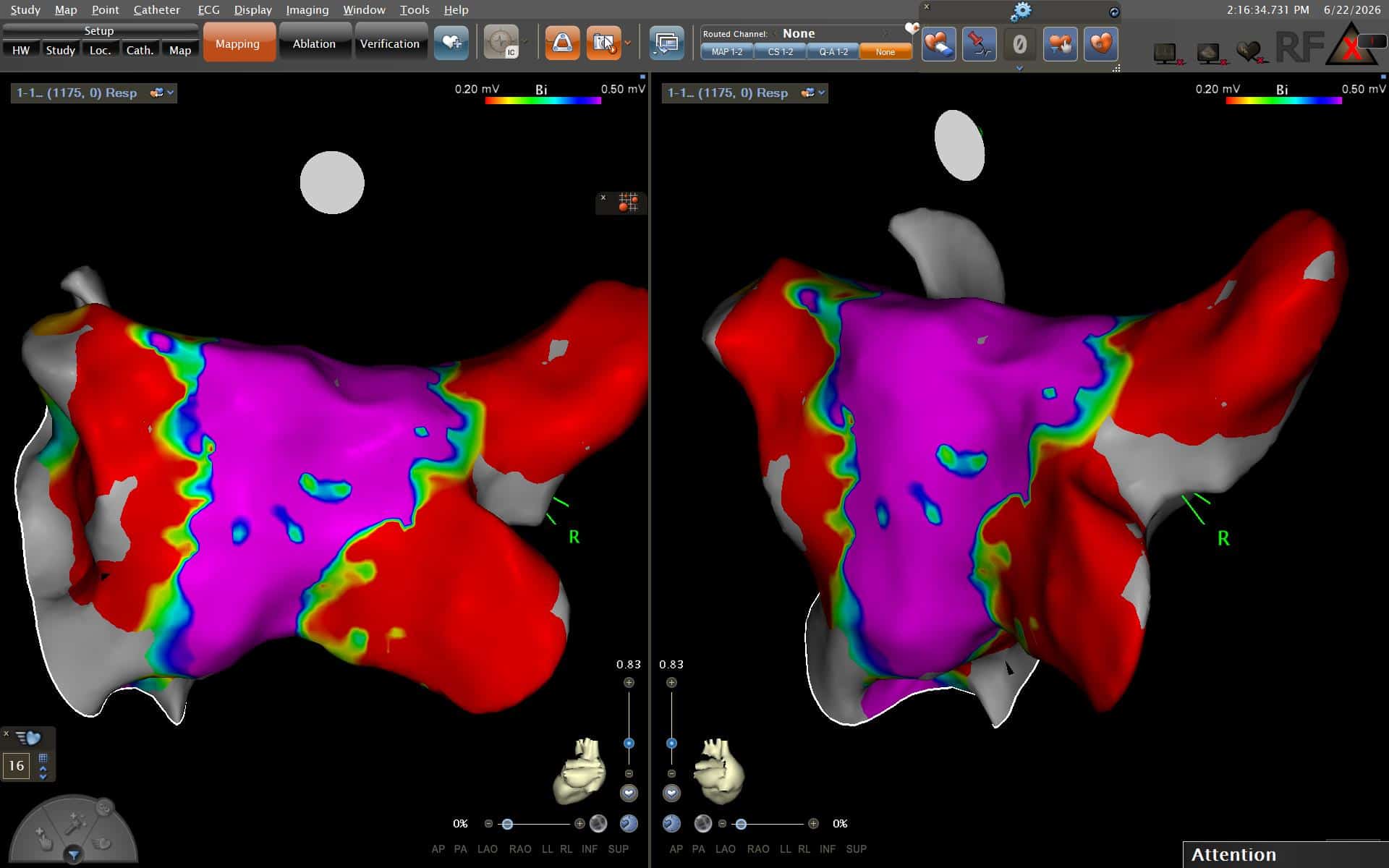
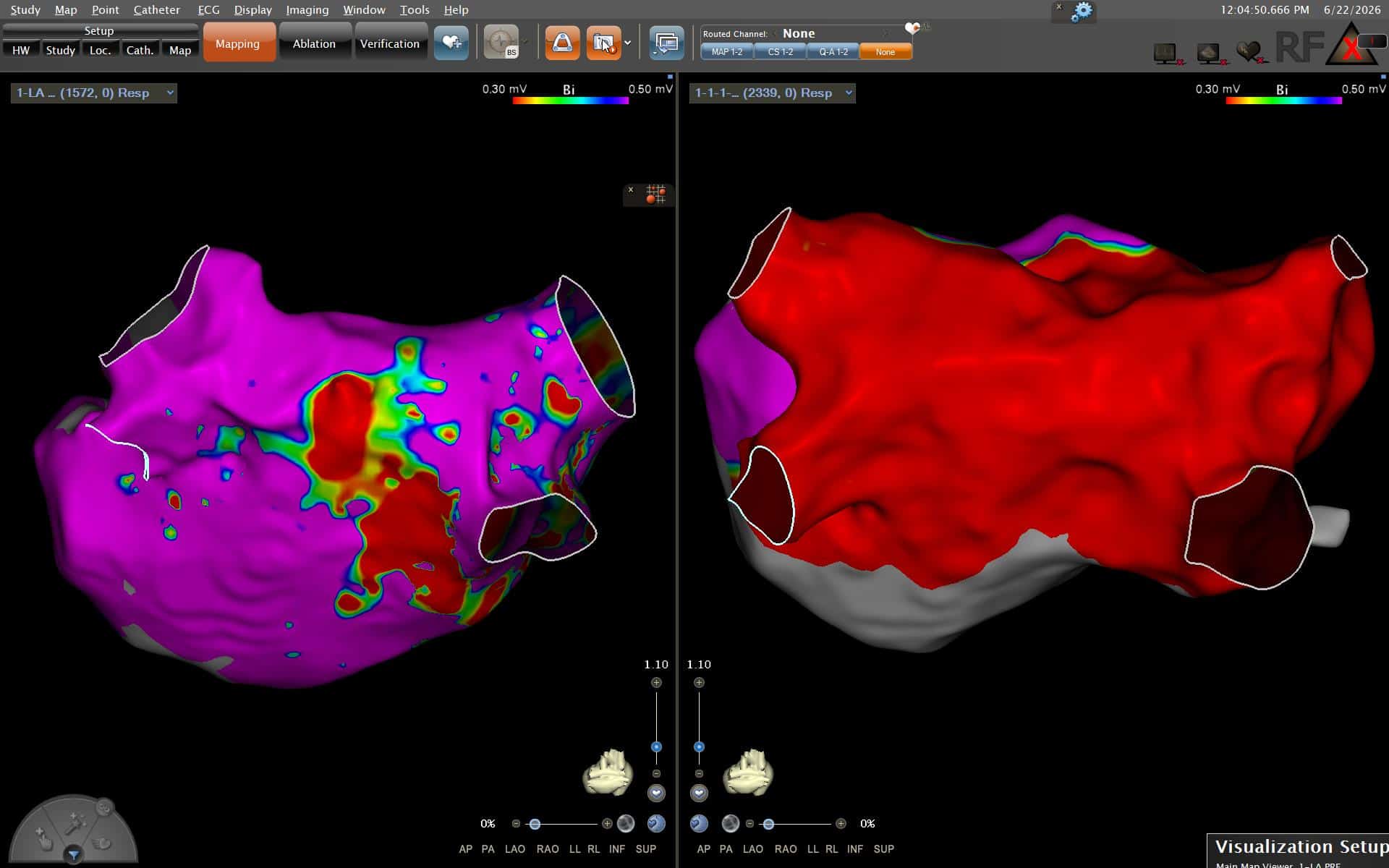
Radiofrequency ablation for AF has evolved significantly. vHPSD delivers energy at 90 watts for just 4 seconds per point. This approach has three important advantages: lesions are more consistent, procedure is faster (shorter time on table), and there is less collateral heating — reducing the risk of thermal injury to adjacent structures like the oesophagus.
The QDot catheter (Biosense Webster) measures the exact force with which the catheter tip touches the heart wall in real time — contact force monitoring. The combination of vHPSD energy and QDot contact force monitoring represents the current standard for RF-based AF ablation at leading centres worldwide.
What this means for you as a patient:
Shorter procedure time. More consistent lesion formation. Real-time confirmation of catheter contact at every point. vHPSD with QDot is a fundamentally more controlled and reproducible approach to pulmonary vein isolation.
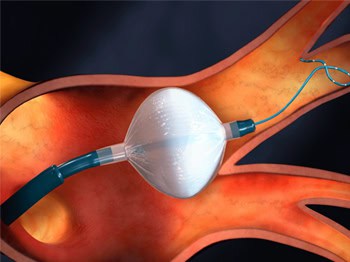
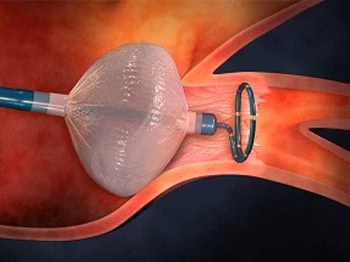
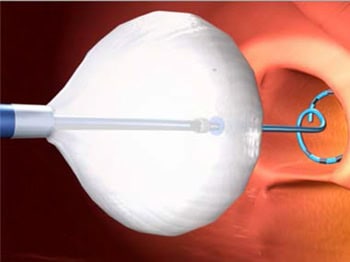
Cryoablation — First-Line for Paroxysmal AF
Cryoablation uses extreme cold to create the ablation lesion. A balloon catheter is advanced to each pulmonary vein and inflated to occlude the vein. Freezing energy creates a circumferential scar that electrically isolates the vein. For paroxysmal AF — AF that starts and stops on its own — cryoablation is an excellent first-line choice. Long-term outcomes are well established across large international trials.


Cryoablation Advantages
-
Consistent circumferential PV isolation
-
Single freeze per vein — efficient procedure
-
Favourable safety profile
-
Strong long-term outcome data in paroxysmal AF
-
Excellent for typical pulmonary vein anatomy
Best Suited For
-
Paroxysmal AF — first presentation
-
Paroxysmal AF — failed anti-arrhythmic drugs
-
Patients with normal or typical PV anatomy
-
Younger patients with symptomatic paroxysmal AF
-
Patients preferring a balloon-based approach
Referring Your AF Patient to HRHF Clinic
HRHF Clinic accepts referrals for AF ablation from across Maharashtra, Goa, Gujarat, and Madhya Pradesh. All procedures are performed personally by Dr. Rajesh Dhopeshwarkar — DM Cardiology (AIIMS), FHRS, CEPS — with over fifteen years of AF ablation experience and the largest series in western India. We offer the complete range of ablation modalities and select the appropriate technique based on the individual patient’s AF type, anatomy, comorbidities, and prior treatment history.
Refer for Ablation Evaluation
-
Symptomatic paroxysmal/persistent AF failing ≥1 AAD
-
Paroxysmal AF — ablation as first-line (guideline supported)
-
Persistent AF with preserved or mildly reduced EF
-
AF with tachycardia-mediated cardiomyopathy
-
Re-do ablation — failed prior PVI at another centre
-
AF with intolerance to anti-arrhythmic drugs
Consider Early Referral
-
Young patient with first-presentation symptomatic AF
-
AF with reduced EF — tachycardia-mediated component suspected
-
Athlete’s AF
-
Newly diagnosed persistent AF — before cardioversion
-
AF with intolerance to anti-arrhythmic drugs
-
Patient asking specifically about ablation options
Common Questions About AF Ablation
Most AF ablation procedures at HRHF Clinic take 2 to 3 hours. Cryoablation is typically at the shorter end of this range. Complex cases or re-do procedures may take longer.
You will receive sedation — you will be comfortable and largely unaware of the procedure. General anaesthesia may be required for AF ablation.
AF ablation has a favourable safety profile in experienced hands. Main risks include vascular access complications, cardiac tamponade (rare), oesophageal injury (rare with vHPSD), and stroke (rare). All risks are discussed in detail pre-procedure.
Ablation significantly reduces AF burden in the majority but does not guarantee permanent cure in all cases. Some patients may require a second procedure. Long-term freedom from AF is higher with ablation than with anti-arrhythmic drugs.
Specific instructions will be given at your pre-procedure consultation. Anti-arrhythmic drugs are typically stopped before ablation; blood thinners are generally continued.
Ready to discuss AF ablation for your patient — or for yourself?
An honest evaluation by a Medtronic national proctor — not a sales pitch. We will tell you whether leadless is the better choice for your specific situation, or whether conventional pacing is more appropriate.